This reports only theestimated efficacy, a projection based on the elaboration of 170 positives (0.5% of the total) out of 43.548 participants in the trial.
The pharmaceutical industry suppresses on the other hand the publication of the data of the guaranteed efficiency, which corresponds only to 30%.
The vaccinee is therefore not fully informed, as the informed consent is MISLEADING, so that every vaccination constitutes an illegal act.
The FDA states: to ensure that a widely deployed COVID-19 vaccine is effective,….. the primary efficacy endpoint estimate is >30%, i.e. only one in three vaccinees becomes immune. Pfizer itself points this out in its publication, basis of the authorization.
The misleading “Advertising” of the 95% “efficacy” e Pfizer) andncourages people to submit to new vaccines, despite possible side effects both immediate (see what is currently happening) and long term (from which the producers exclude themselves: see Pfizer consent).
Likewise the current political pressure to have to be vaccinated to be able to travel, continue to work etc. is in stark contrast to theEuropean Parliament resolution 2361 of 27/01/2021, which declares: “7.3.1. ensure that citizens are informed that the vaccination is NOT mandatory and that no one is politically, socially, or otherwise pressured to get themselves vaccinated, if they do not wish to do so themselves;
7.3.2. ensure that no one is discriminated against for not having been vaccinated, due to possible health risks or not wanting to be vaccinated”.
This resolution is probably the result of having realized that forcing the population to have a vaccine which is not very effective and not very safe, would make the suspicion of a political- medical-economic collusion a certainty signed: “European Community”.
As Henry Gadsden, at that time CEO of Merck, said thirty years ago in an interview with Fortune (the second most important economic magazine in America):
Our dream is to produce drugs for healthy people.
This would allow us to sell them to everyone like the Chewing gum giant Wrigley’s.
The trials are going in the same direction, aiming to produce vaccines for healthy childrenfrom 6 months to 12 years of age, precisely from AstraZeneca. There is no scientific evidence that children get sick or infect others.
That is why all this constitutes a CRIME AGAINST HUMANITY.
PfizerBioNTech, in its admission statement to the FDA explicitly stated that: the actual efficacy of the vaccine is higher than 30%(Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine, 2020). Therefore it is guaranteed that only one vaccinated person in three becomes immune, not 95%.
The 95% efficacy refers to another statistical processing data used in medical statistics. As soon as 170 (only 0.5%) of the total 43,548 participants in the Pfizer study became positive, the trial was ended (there was no mention of antibody titre etc.).
Of these 170 participants, 162 were in the unvaccinated group and 8 in that of the vaccinated. If you put 162 in relation to 8 you get a quotient = 95%, which in English is called: “efficacy” (relative efficiency), which definitely not to be confused with “efficiency” (absolute efficiency) (according to Pfizer-BioNTech at least 30% become immune).
These famous 30% are required by the FDA to accept vaccines produced at a time of emergency (Food and Drug Administration. https://www.fda.gov/media/139638/download), way below normal standards.
A statistical model of common consent has been created(political-medical-industrial) in order to give everyone (more than 200 centres worldwide) the authorization for trials, production and marketing of the vaccines without any basis of valid medical statistics.
At this point we need to make some elementary statistical observations:
Setting up a statistical study in medicine requires criteria, so that it is significant not only statistically but also clinically relevant.
The criteria are as follows:
Unambiguous definition of the single events of the study (the definition e.g. of “Covid patient” in the Pfizer study is clinically totally insufficient: see attachment),
Determination of the level of significance: in medicine the p<0.05 level is mostly used (which allows for only one error in 20 forecasts/tests)
Determination of the desired benefit to be achieved (e.g. how low does the blood pressure have to drop to justify the administration of a drug, or: how effective does the vaccine have to be to be able to administrate it).
The necessary number of participants is calculated from these last two criteria (2-3). Choosing a higher number a difference will be seen, but not more clinically significant. This appears to be a contradiction. But increasing the number of samples serves only to put the insignificant efficacy of a vaccine/drug on the front page, which however in practice produces more negative than positive effects. In the case of the Covid vaccine this means that a substantial part of the world is subjected to an ineffective vaccine (statistically it guarantees 30% protection) connected to all the associated dangers for those vaccinated besides the economic, administrative etc. efforts.
The statement, that 95% of those vaccinated is protected from Covid infection, is maybe due to a mistaken translation from the specific terms in English.
But it is also possible, that the realization, that they had not interpreted the data provided by the drug companies correctly, prompted the authorities to carry out vaccinations, omitting two basic principles for vaccinations:
Determination of the actual infective state: it is mandatory to take a swab immediately before vaccinationto avoid serious adverse events caused by a double entry into the body of two similar antigens (virus and vaccine),
Determination of the actual state of immunity: it is mandatory to carry out a serological test before vaccination. Omitting this, maybe they hope in the end to be able to add the number of naturally immune tothat of thevaccination, interpreting this result as the success only of thevaccination, putting a tombstone on the errors made and also on the general number of naturally immune. If in the end the immunity is still not that promised, the variants of the virus will be blamed, now presented daily as one of the main “enemies”.
The statement: that the Pfizer vaccine “prevents up to 95% of adults aged 16 and over from developing the Covid-19 disease” is misleading, which exposes people to submit to vaccines on the one hand unsafe because of the shortened approval and on the other not very effective (30% of immunization), as scientifically proven.
The European Parliament resolution 2361 (27/01/2021):
“7.3.1. ensure that citizens are informed that the vaccination is NOT mandatory and that no one is politically, socially, or otherwise pressured to get themselves vaccinated, if they do not wish to do so themselves;
7.3.2. ensure that no one is discriminated against for not having been vaccinated, due to possible health risks or not wanting to be vaccinated”.
has exempted politicians etc. from the risk of being accused of promoting a vaccination which is not very effective but full of potential risks. The suspicion of collusion between politicians and the pharmaceutical industry would have become a certainty.
Appendix:
The definition “suffering from Covid-19” applied by the Pfizer trial is based on epidemiological evidence, on the presence of multiple symptoms common to many other similar diseases and on confirmation by positive swab (by PCR).
PCR does not show that someone is sick … and does not show that what has been found would have been harmful.
With PCR, if it is done well, you can find almost anything in everyone.
However the latter does not show an ongoing infection, but onlycontact with the coronavirus. A person who was with smokers, is not necessarily a smoker (the transmission of the coronavirus is similar to that of passive smoke).
The confirmation of an entry into the body and the reaction of the body to the virus is shown only by the presence of specific antibodies in the blood (serological test).
The search for these antibodies
was not done so as not to lose the number of “positives” necessary to be able to present the vaccine as soon as possible,
is not even done on those currently vaccinated (very serious medical error), so as to lose the traces of a previous immunity and not to have to admit that there have been very many false positives because of swabs, which have created tremendous economic, psychological etc. harm.
DER IMPFBETRUG
Die Behauptung, “ nach derzeitigem Kenntnisstand bieten die COVID-19-mRNA-Impfstoffe eine hohe Wirksamkeit von bis zu 95 % (Comirnaty®) bzw. 94 % (COVID-19 Vaccine Moderna) (Aufklaerungsblatt Robert Koch Institut) ist unvollstaendig und bewust irrefuehrend.
Es wird nur auf die geschaetzte Wirksamkeit hingewiesen, die sich auf die Auswertung von 170 Coronainfizierten von 43548 Studienteilnehmern (<0.5%). Es wird jedocj bewust die garantierte Wirksamkeit verschwiegen, die bei 30% liegt
Der Impfkandidat wird somit nicht nur unzureichend, sondern IRREFUEHREND aufgeklaert, weswegen jede Impfung unrechtmaesig ist.
Die FDAverlangt: “um zu gewaehrleisten, dass eine Covid-Impfung wirksam ist ….ist eine Wirksamkeit von mindestens 30% erforderlich”. Dies heisst, dass nur einer von drei Geimpften immun werden muss. Pfeizer selbst weist darauf in seiner Veroeffentlichung hin, die die Basis der Zulassung war.
Die irrefuehrende “Werbung” der 95% Wirksamkeit (Pfeizer) und 60% (AstraZeneca)auch mittels der Medien, veranlasst die Menschen, sich mit vollstaendig neuen Stoffen impfen zu lassen. All dies trotz der moeglichen unmittelbaren Nebenwirkungen (siehe AstraZeneca etc.) und der Spaetwirkungen, fuer die die Produzenten keine Verantwortung uebernehmen (siehe Patientenaufklaerung Robert Koch Institut).
Weiterhin steht der politische Impfdruck (um reisen, arbeiten etc. zu koennen) im deutlichem Widerspruch zur Resolution 2361 vom 27/01/2021 des Europaeischen Parlaments, die fordert:
„7.3.1. sicherstellen, dass Bürgerinnen und Bürger informiert werden, dass die Impfung NICHT verpflichtend ist und niemand politisch, sozial oder auf andere Weise unter Druck gesetzt wird, sich impfen zu lassen, wenn sie es nicht selbst möchten“.
7.3.2 sicherstellen, dass niemand diskriminiert wird, weil er aufgrund von möglichen Gesundheitsrisiken oder weil er es möchte, nicht geimpft wurde
Diese Resolution ist wahrscheinlich aus der Einsicht geboren, dass bei Impfzwang aller Buerger mit wenig wirksamen und wenig sichere Stoffen, der Verdacht einer politischen – medizinischen- oekonomischen Absprache (unterzeichnet Europaeische Union) zur Gewissheit werden koennte.
Wie sagte bereits vor 30 Jahren der derzeitigen Chef des US-Pharmariesen Merck Henry Gadsden in einem Interview mit der Zeitung Fortune:
:
Unser Traum ist, Arzneimittel fuer Gesunde zu entwickeln.
Dies wuerde es uns erlauben, sie jedem wie den Chewing gum giant Wrigley’s zu verkaufen.
In diese Richtung geht die Studie, die Impfstoffe fuer gesunde Kindern von 6 Monaten bis 12 Jahren entwickeln soll, und gerade von AstraZeneca. Wissenschaftlich gibt es zur Zeit keinerlei Evidenz, dass Kinder an Coronavirus erkranken oder als Uebertraeger gelten. Deswegen ist dies ein VERBRECHEN AN DIE MENSCHLICHKEIT.
ARTIKEL
Die Behauptung, “ nach derzeitigem Kenntnisstand bieten die COVID-19-mRNA-Impfstoffe eine hohe Wirksamkeit von bis zu 95 % (Comirnaty®) bzw. 94 % (COVID-19 Vaccine Moderna) (Aufklaerungsblatt Robert Koch Institut)ist eine der groessten Falschmeldungen in der juengeren Geschichte der Medizin.
Pfeitzer BioNTech hat in seinem Artikel zur Zulassung bei der FDA nur erklaert, dass die Wirksamkeit des Impfstoffes ueber 30%liegt,(Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine, 2020).Somit wird nur garantiert, dass einer von drei eine Immunitaet entwickelt, nicht 95%.
Die Wirksamkeit von 95% ist nur eine statistische Vorhersage aufgrund der Auswertung eines Bruchteiles des Studienkollektives. Sobald von den insgesamt 43.548 Teilnehmer der Pfeizerstudie 170 an Coronavirus (0.5%) erkrankt waren (jedoch ohne sierologische Bestaetigung), wurde die Studie beendet.
Von diesen 170 Erkrankten kamen 162 aus der Plazebogruppe und 8 aus der Impfgruppe, woraus sich der Quozient von 95% ergibt. Dieser drueckt die “efficacy” (relative Wirksamkeit), die jedoch nicht mit der “efficenzy” (absolute Wirksamkeit)aus, die bei Pfizer-BioNTech bei 30% liegt.
Diese 30% werden von der FDA gefordert fuer Impfstoffe in Notfallzulassung https://www.fda.gov/media/139638/download), deutlich geringer ald fuer andere Impfstoffe.
Es wurde ein statistisches Modell in allgemeiner Ueberinstimmung (Politik, Medizin, Industrie) entwickelt um fast allen (mehr als 200 Zentren in der Welt) die Moeglichkeit zur Erforschung, Herstellung und Vertrieb von Impfstoffen zu erlauben, ohne jeglicher Grundlage fuer Medizienische Statistik.
Hierzu muessen ein paar Ueberlegungen ueber die Basis der Statistik angestellt werden:
Der Aufbau einer Statistischen Studie in der Medizin benoetigt bestimmte Kriterien, damit selbige nicht nur eine statistische sondern auch eine klinisch relevante Bedeutung hat.
Dies sind die Kriterien:
Eindeutige Definition der einzellnen Bestandteile der Studie (die Kriterien der Definition: Covid-Patient sind voellig unzureichend (siehe Anlage),
Bestimmung des Signifikanzniveaus: in medizinischen Untersuchungen wird dies auf < 0.05 angesetzt, was nur einen Fehler auf 20 Vorhersagen/Tests erlaubt.
Bestimmung der erhofften klinisch rilevanten Veraenderung, die die Anwendung des Arzneimittels etc. gerechtfertigt.
Mittels diesen beiden letzten Kriterien (2-3) wird der Strichprobenumfang festgelegt. Wird ein groesserer Umfang gewaehlt, wird eine Wahrscheilichkeit festgestellt werden, die jedoch klinisch nicht bedeutend ist. Dies erscheint ein Widerspruch, aber den Stichprobenumfang zu erhoehen, dient nur dazu, eine unbedeutende Wirksamkeit eines Impfstoffes/Arzneimittels in den Vordergrund zu stellen. Dies alles obwohl in Wirklichkeit nur mehr Nebenwirkungen als ein positiver Effekt erzeugt wird. Im Falle der Coronaimpfung bedeutet dies, dass ein grosser Anteil der Weltbevoelkerung einer wenig wirksamen Impfung (30% Immunitaet) verbunden mit all den Risiken unterzogen wird.
Die Behauptung, dass 95% der Gemipften vor Coronaerkrankung geschuetzt sind ist wahrscheinlich aus einer fehlerhaften Uebersetzung des spezifische englischen Ausdruckes entstanden.
Es ist jedoch moeglich, dass es die Einsicht ist, die Daten der Pharmaindustrie nicht richtig interpretiert zu haben, die die Regierungen dazu gebracht zu haben, die Impfungen durchzufuehren. Bei der Impfdurchfuehrung werden zwei elementare Grundlagen straeflich uebergangen:
Bestimmung einer vorliegenden Coronainfektion: es ist unerlaesslich einen Abstrich unmittelbar vor der Impfung durchzufuehren, um eine bestehende Infektion nachzuweisen, da ein zweifacher Kontakt mit aehnlichen Antigenen (Virus und Impfung) zu unvorhersehbaren Reaktionen fuehren kann
Bestimmung des Immunstatus des Patienten: es ist unerlaesslich, einen sierologischen Befund ueber den Immunstatus des Patienten zu erhalten, um auch mehr ueber die Verbreitung des Virus zu erfahren. Dies wird wahrscheinlich auch deswegen unterlassen, um die geringe Impfwirkung mit der natuerlich bereits erhaltenen Immunitaet summieren zu koennen und dies als Erfolg der Impfung praesentieren zu koennen. Somit kann man einen Grabstein auf die begangenen Fehler und die natuerlich erworbene Immunitaet legen. Wenn allerdings die Immunitaet auch dann nicht die erhoffte ist, so kann man immer noch die Schuld auf die Varianten des Virus schieben, die mittlerweile jeden Tag als eine der Hauptfeinde angeprangert werden.
Die Behauptung, dass der Impfstoff Pfeizer “zu 95% der Erwachsenen ueber 16 Jahre verhindert, die Krankheit Covid-19 zu entwickeln, ist irrefuehrend: und bringt die Menschen dazu, sich Impfungen zu unterziehen, die einerseits unsicher sind aufgrund der kurzen Zulassungszeit, und andererseits, da sie wenig wirksam sind (30% Immunitaet) wie allerseits wissenschaftlich bestaetigt.
Die Resolution des europaeischen Parlamentes 2361 (27/01/2021):
„7.3.1. sicherstellen, dass Bürgerinnen und Bürger informiert werden, dass die Impfung NICHT verpflichtend ist und niemand politisch, sozial oder auf andere Weise unter Druck gesetzt wird, sich impfen zu lassen, wenn sie es nicht selbst möchten“.
7.3.2 sicherstellen, dass niemand diskriminiert wird, weil er aufgrund von möglichen Gesundheitsrisiken oder weil er es möchte, nicht geimpft wurde
hat die Politiker vom Risiko der Anklage befreit, die Buerger zu einer unsicheren und unwirksamen Impfung zu verpflichten mit allen seinen Folgen. Dies haette den Verdacht der Vernetzung von Politik, Medizin und Industrie zur Gewissheit werden lassen.
ANHANG:
Die Diagnose “Coronakranker”, die von den Impfstudien angewandt wurde, basiert auf epidemilogische Kriterien, klinische weitverbreiteten Syptomen und einen positiven Rachenabstrich (mittels PCR, der molekulare Test).
Der Nobelpreisstraeger, Erfinder der PCR, Kary Mullis selbst hatte erklaert:
Die PCR beweist nicht, dass jemand erkrankt ist …..und beweist nicht, dass das, was man gefunden hat, Schaden haette anrichten koennen.
Wenn die PCR gut gemacht ist, kann man fast alles bei fast jedem finden.
Es wird tatsaechlich keine Infektion nachgewiesen, sondern nur ein vorhergegangener Kontakt mit einem Coronaauscheider: jemand, der mit einem Raucher in Kontakt war, ist selber noch kein Raucher. (die Uebertragung des Coronavirus ist vergleichbar mit der des Passivrauches). Die Bestaetigung des effektiven Eindringens in den Koerper erfolgt nur mittels Nachweis von spezifischen Antikoerpern im Blut erfolgt.
Die Suche nach diesen Antikoerpern erfolgt jedoch nicht:
Um die Impfung unerlaesslich erscheinen zu lassen,
Um die natuerlich bereits erworbene Immunitaet nicht aufzuzeigen. So muss man nicht zuzugeben, dass eine Vielzahl von falschen Positiven (vor allem Kinder) sich einer Quarataene unterziehen mussten, mit all den enormen finanziellen, psychischen und weiteren Schaeden.
Questa riporta solo l’efficacia stimata, una proiezione basandosi sulla elaborazione di 170 positivi (0.5% del totale) su 44.000 partecipanti alla sperimentazione.
L’industria farmaceutica sopprime dall’altro canto la pubblicazione dei dati dell’efficacia garantita, che corrisponde solo al 30%.
Il vaccinando viene pertanto informato in maniera incompleta, essendo il consenso informato INGANNEVOLE, per cui ogni vaccinazione costituisce un atto ilegitimo.
La FDA, dichiara: “per garantire, che un vaccino Covid-19 è effettivo …viene richiesto una efficienza del 30%”. Cioè solo uno su tre vaccinati diventa immune. La Pfeizer stesso lo sottolinea nella sua pubblicazione, base dell’autorizzazione.
La “Pubblicità” ingannevole del 95% (Pfeizer), e del 60% (AstraZeneca) di “efficacia” (sostenuta anche da tutte le media) induce le persone, di sottoporsi a dei vaccini completamente nuovi. Tutto questo avviene nonostante gli effetti collaterali immediati (vedi quello che sta succedendo attualmente) ed a lungo termine (delle quali i produttori stessi si escludono: vedi consenso Pfeizer).
Inoltre la pressione politica attuale, di doversi vaccinare per poter viaggiare, per poter continuare a lavorare ecc., è in netto contrasto alla risoluzione 2361 del Parlamento Europeo del 27/01/2021, che decreta: “7.3.1 garantire che i cittadini siano informati che la vaccinazione NON è obbligatoria e che nessuno è politicamente, socialmente o altrimenti sotto pressione per vaccinarsi, se non lo desiderano da soli; 7.3.2 garantire che nessuno sia discriminato per non essere stato vaccinato, a causa di possibili rischi per la salute o per non voler essere vaccinato”.
Questa risoluzione è probabilmente il risultato della presa di coscienza, che costringere la popolazione ad un vaccino poco efficace e poco sicuro, farebbe diventare il sospetto di una collusione politico – medico – economico una certezza firmato: “Comunità Europea”.
Come diceva trent’ anni fa l’allora direttore della Merck, in una intervista al Fortune (seconda rivista economica più importante dell’America),
Henry Gadsden:
Il nostro sogno è quello, di produrre farmaci per le persone sane.
Questo ci permetterebbe di venderli a chiunque come il Chewing gum giant Wrigley’s.
In tale senso va la sperimentazione, che mira a produrre vaccini per bambini sani da 6 mesi a 12 anni, proprio dall’AstraZeneca. Scientificamente non c’è alcuna evidenza, che bambini si ammalano o infettano altri.
Perciò tutto questo costituisce un CRIMINE ALL’UMANITA’.
La Pfeitzer BioNTech, nel suo articolo base alla amissione all’FDA ha esplicitamente dichiarato che: l’efficacia effettiva del vaccino è superiore del 30%(Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine, 2020).Pertanto viene garantito, che solo un vaccinato su 3 diventa immune, non il 95%.
L’efficacia del 95% si riferisce su un altro dato di elaborazione statistica utilizzato nell’ambito della statistica medica e si basa solo su una proiezione possibile. Appena sui complessivi 43.548 partecipanti allo studio Pfeizer 170 (solo il 0.5%) erano diventati positivi, la sperimentazione si era conclusa (non si parlava di titolo anticorpale ecc.).
Di questi 170 partecipanti 162 erano del gruppo dei non vaccinati e 8 di quello dei vaccinati. Mettendo i 162 in rapporto con i 8 si ottiene un quoziente = 95%, quale viene chiamato in inglese: “efficacy” (efficienza relativa), che però non deve essere assolutamente confuso con la “efficenzy” (efficienza assoluta)(sec. Pfizer-BioNTech almeno il 30% diventa immune).
Questi famosi 30% sono richiesti dalla FDA per accettare vaccini prodotti in fase di emergenza (Food and Drug Administration. https://www.fda.gov/media/139638/download), molto inferiore ai standard normali.
E’ stato creato un modello statistico di comune consenso (politico – medico – industriale) ai fini di dare a tutti (più di 200 centri nel mondo) l’autorizzazione di sperimentazione, produzione e commercializzazione di vaccini senza alcuna base di statistica medica valida.
A questo punto bisogna fare qualche osservazioni elementari di statistica:
L’impostazione di uno studio statistico in medicina richiede dei criteri, affinché avesse una importanza non solo statisticamente ma anche clinicamente rilevante.
I criteri sono i seguenti:
Definizione univoca dei singoli eventi dello studio (la definizione ad. es. di “paziente Covid” dello studio Pfizer è clinicamente completamente insufficiente: vedi allegato),
Determinazione del livello di significatività: in medicina viene maggiormente usato il livello p<0.05 (che ammette solo un errore su 20 previsioni/esami)
Determinazione del auspicato benefico da raggiungere (ad es. per quanto si deve abbassare la pressione arteriosa per giustificare la somministrazione di un farmaco, oppure: quanto deve essere efficace il vaccino per poterlo somministrare).
Da questi ultimi due criteri (2-3) viene calcolato il numero necessario dei partecipanti. Scegliendo un numero più elevato si evidenzierà si una differenza, ma non più clinicamente significativa. Questo sembra una contraddizione. Ma aumentare il numero dei campioni serve solo per mettere in prima pagina l’efficacia insignificante di un vaccino / farmaco, che però all’atto pratico produce più effetti negativi che positivi. Nel caso del vaccino Covid significa, che una considerevole parte del mondo viene sottoposta ad una vaccinazione poco efficace (statisticamente garantisce una protezione al 30%) connesso con tutti i pericoli collegati per i vaccinanti oltre ai sforzi economici, amministrativi, ecc.
L’affermazione, che il 95% dei vaccinati è protetto dall’infezione da Covid è forse dovuta ad una errata traduzione dei termini specifici dall’inglese.
E’ però pure possibile, che la presa di coscienza, di non aver interpretato in maniera corretta i dati forniti dalle dite farmaceutiche, ha indotte le autorità di effettuare le vaccinazioni omettendo due principali fondamenta per le vaccinazioni:
Determinazione dello stato infettivo attualmente in atto: è d’obbligo di eseguire un tampone immediatamente prima della vaccinazione per evitare eventi avversi gravi a causa di un duplice ingresso nel corpo di due antigeni simili (virus e vaccino),
Determinazione dello stato di immunità attualmente in atto: è d’obbligo di eseguire un esame sierologico prima della vaccinazione. Omettendo quest’ultima, forse si spera alla fine di poter sommare il numero dei immuni per via naturale a quella da vaccinazione, interpretando tale risultato come successo solo della vaccinazione, mettendo una pietra tombale sui errori commessi ed anche sul numero generale dei immuni naturali. Se alla fine ancora l’immunità non è quella promessa, la colpa verrà assegnata alle variazioni del virus, ormai presentate ogni giorno come i principali “nemici”.
L’affermazione: che il vaccino Pfizer “impedisce al 95% degli adulti dai 16 anni in poi di sviluppare la malattia covid-19” è una affermazione ingannevole, che espone le persone a sottoporsi a dei vaccini da un lato insicuri a causa dell’approvazione abbreviata e dall’altro lato poco efficaci (30% di immunizzazione), come scientificamente dimostrato.
La risoluzione del Parlamento Europeo 2361 (27/01/2021), di non imporre alcun obbligo per le vaccinazioni, ha esentato i politici ecc. dal rischio, di essere responsabili dei probabili effetti collaterali gravi e di venire accusati, di promuovere una vaccinazione poco efficace ma ricca di potenziali rischi. Il sospetto di una collusione tra politica ed industria farmaceutica sarebbe diventata certezza.
Appendice:
La definizione “affetto da Covid-19” applicato dalla sperimentazione Pfizer si basa su evidenze epidemiologiche, sulla presenza di sintomi molteplici comuni a tante altre affezioni simili e sulla conferma tramitetampone positivo (tramite PCR).
LaPCR non dimostra, che uno è malato… e non dimostra, che quello, che si ha trovato, avrebbe recato danno.
Con la PCR, se fatta bene, si può trovare quasi tutto in ognuno.
Viene dimostrato solo che la persona è venuta a contattocon il coronavirus, ma non che è stato infettato con una risposta anticorpale, rilevabile con il test sierologico. Una persona, che era insieme con un fumatore, non è per forza fumatore (la trasmissione del Coronavirus è paragonabile a quello del fumo passivo).
La conferma di un effettivo ingresso nel corpo e la reazione del corpo al virus viene rilevato solo dalla presenza nel sangue di anticorpi specifici (esame sierologico).
La ricerca di questi anticorpi
non fu fatta per rendere il vaccino indispensabile,
non viene fatto neanche ai attuali vaccinanti (gravissimo errore di medicina), ai fini di far disperdere le tracce di una immunità già avvenuta precedentemente. Inoltre non si dovrà ammettere, che ci sono stati tantissimi falsi positivi a causa dei tamponi, che dovevano fare la quarantena (specie i Bambini), il che ha creato danni economici, psicologici ecc. immensi.
The four elimination pathways and Coronavirus or:
Medicine is not a science but an opinion.
The obligation for masks is considered one of the most effective measures to combat the coronavirus pandemic. This measure is imposed, like many others, only for populist political reasons and is not only completely ineffective with regard to a reduction in the transmission of the virus, but also constitutes a serious danger to the health of anyone wearing the mask (1) (European Centre for Disease Prevention and Control 2020). This problem is sidetracked, deliberately creating great confusion among the sick, the dead, the HIV-positive, the healthy carriers, the asymptomatic, the positive etc.
In the end the contagiousness index was introduced (Robert Koch Institute) as the supreme judge of good and evil, which arbitrarily divides countries into zones of good and bad citizens, the latter to be ruthlessly punished. All this happens with no scientific basis and is statistically unacceptable, but the hunt for positives with all available means (immune App etc.) has become one of the “main weapons in the fight against the Coronavirus”. Those discovered positive and their families are put under house arrest and pilloried, as if they were criminals.
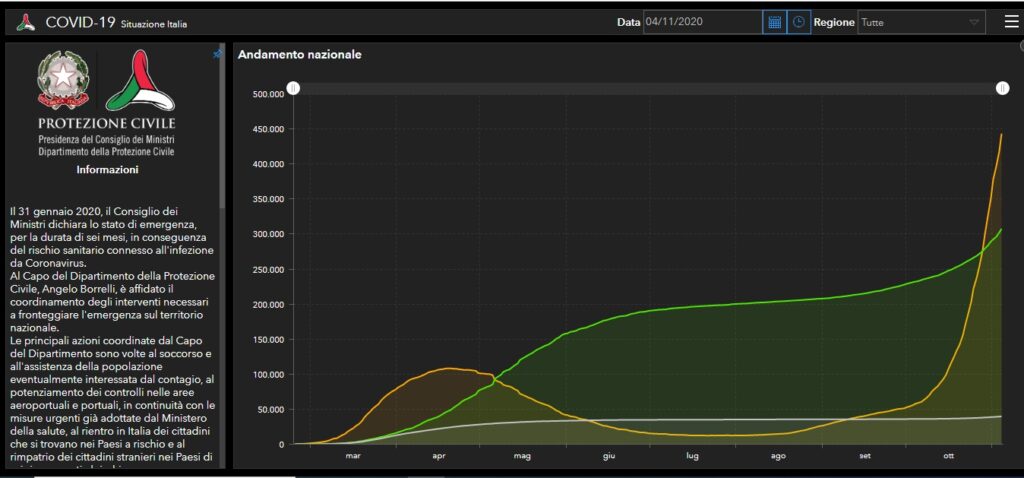
But this hunt makes no sense, as the contagiousness index is completely unrelated to mortality, as shown by the statistics issued by the Italian Ministry of Health/ Ministero della Salute Italiano on 4/11/20 (2).
Curve – yellow: currently positive, green: recovered, grey: deaths
BUT WHAT IS WRONG WITH MASKS?
I’ll explain it in a nutshell.
Our body has four elimination pathways for noxious substances: urinary tract (urine), digestive tract (feces), skin (perspiration) and the lungs (respiration). This last pathway, important with regard to coronavirus transmission, must guarantee both the oxygen/carbon dioxide exchange and the ventilation of the respiratory tracts, the nasal and paranasal sinuses and the middle ear.
If this or any other pathway is interrupted or reduced, the body gets progressively intoxicated and damaged even irreversibly.
And now we come to masks:
Masks in no way protect against coronavirus infection as the means of transmission is exclusively aerial by aerosols (3) and not through droplets or contact.
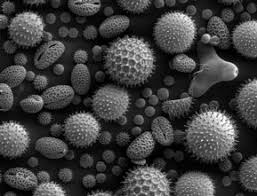
The Coronaviruses have a superimposable shape to that of various pollens (one of nature’s wonders) but they are much smaller and are transmitted in the same way, suspended and transported by air. If they land on fertile ground (for the coronavirus the peripheral airways, i.e. the bronchioles) they take root and then multiply.
CoronavirusPollen from a peanut bush
Their dimensions are also comparable to those of smoke particles, they get to the alveoli and are then inhaled and exhaled. This is the difference to droplet particles, which having a diameter about 60 times higher, are picked up by the upper respiratory tracts.
The Coronavirus’ gateway to the body and its replication finally take place at the level of the peripheral airways (bronchioles), where they induce an inflammatory response mediated by antibodies similar to allergic asthma. This is why the severity of the disease does not primarily depend on the damage caused to the organism by the virus, but on the damage caused by the immune system to the organism (4), which is why cortisone was the first choice drug in aggravated cases at the beginning of the pandemic.
The modes of falling ill with coronavirus are comparable to those of falling ill from passive smoking. Coming into contact with people who transmit coronavirus is the same as coming into contact with smokers. The harmful agent is inhaled in the same way and the dangerous load for the organism only takes place in closed, badly ventilated environments.
In this respect the Robert Koch Institute has confirmed that transmission of the virus in the open is highly improbable (RKI).
Masks are very dangerous because they greatly reduce the aeration of the lungs.
Once respiratory system patients were sent to the mountains or the sea to exhale the unhealthy air and inhale clean air, whereas now they are provided with masks and the exhaled air (which contains a high number of viruses during the infectious phase) cannot disperse in the open air but is retained by the mask and subsequently inhaled.
“Put on your costume”
In this respect masks oblige people to infect themselves more and more (as if one smoked under the mask), condemning them to an increasingly serious risk to their health and producing severely ill patients.
And so, breath by breath, people reduce their chances of survival. HOORAY FOR MEDICINE!
Unfortunately medicine is not a science, but an opinion. Day by day many opinions (political, economic, populist etc.) interfere on the orientation of medicine, also with compliant experts in the medical sphere. In arithmetic, (which is a science) one and one makes two (1+1=2), in medicine (which is an opinion) 1+1 does not always make 2, it eventually makes 3, 4 or 18, 24, maybe better 42-2, according to the current opinion.
With the current government measures we are actually forced to take refuge in closed places, right where we get infected and then we are forced to endure serious or very serious harm caused by the obligation for masks. We are taken right there, young and old, where we don’t want to end up, in the arms of the angel of death.
APPENDIX:
Ceterum censeo, Cartaginem esse delendam, thus Cato, the Censor finished each of his speeches at the Senate.
In this sense this contribution ends with:Ceterum Censeo, that the situation is not of a medical but a political/economic nature, public good and health have nothing to do with it, common people are nothing but cannon fodder:
Because there is a daily organized disinformation of the population regarding mortality, lethality, contagiousness index, deceased, newly infected, re-infection, asymptomatic, healthy carriers, positives. The latter are pursued with all the means at the disposal of the state, as if they were criminals. But this hunt makes no sense, as the contagiousness index is completely unrelated to mortality, as shown by the statistics issued by the Italian government on 4/11/20 (A).
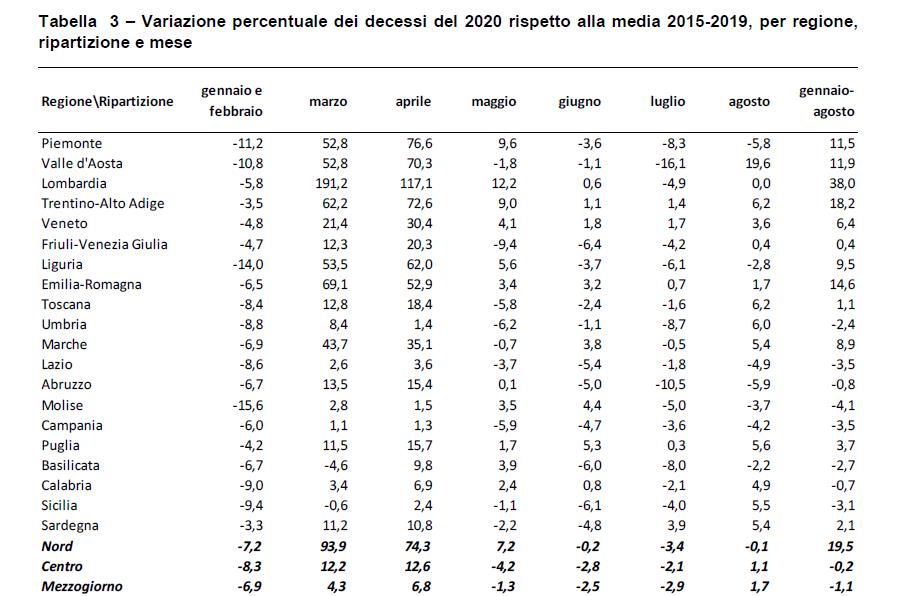
Because disastrous news is broadcast every day regarding the pandemic, even though this year (e.g. in Italy, in Germany the relevant data is not available) there has not been a statistically significant rise in mortality compared to the period 2015-2019. From May-August there was even a reduction in mortality compared to the five previous years by 1.6% (ISTAT Report, National Institute of Statistics 22/10/2020 (Table 1)(B).
Because the statistics released by the media predict a significant increase in deaths from coronavirus with distressing forecasts for the future, (“soon over 1,000 deaths a day”), even though the lethality of Coronavirus is estimated at 0.14% against the 0.10 of common ‘flu (WHO 14/10/20)(C). Possibly because even patients without laboratory confirmation are included in the deaths with only a suspected diagnosis (as a result of medical or epidemiological evaluation) (Report of the National Health Insitute (ISS), n.49/2020,8/6/20, note 1)(D), or because the statistical elaboration was carried out on limited groups of patients (4942 of 31.573 deaths from Coronavirus to 25/05/2020), or because inappropriate terms of definition were used. The term “directly responsible for death”, means that the death would not have beenverified if the SARS-CoV-2 infection had not intervened, although often overlapping other pre-existing conditions, and their complications. (Report from the “National Institute of Statistics on16/7/2020: Impact of the Covid-19 epidemic on mortality: Causes of death of SARS-CoV-2 positives, note 2)(E).
At the moment almost all the hospitals in almost all Europe are nearly full of Coronavirus patients, even though current mortality is much lower than in the spring. Also the capacity of hospital beds for coronavirus patients has increased since then. This could serve to recover the deficit of hospitals caused by the dramatic reduction in hospital admissions due to the pandemic (the deficit in the first 4 months in Italy is 3.5 bilions of Euro: Report ALTEMS) (F). In this way the Budget can be met, so as not to remain insolvent. (“Coronavirus rettet die Kliniken, aber die Pleitegefahr bleibt hoch” = the coronavirus crisis saves the hospitals, but the risk of bankruptcy remains high. Das Handelsblatt ) (G). In Germany the state pays the hospitals about 700 euro for every unoccupied bed, to keep it free for the eventual second wave of the pandemic. All this because direct subsidies at EU level are no longer permitted. If someone cannot uphold their financial obligations, they have to declare insolvency, a disaster for public healthcare.
Because in March wide-spectrum trials of antiviral drugs like Remdesivir (Solodarity etc.) were authorized globally, where the control group did not receive any specific pharmacological drug, which actually should have been cortisone. In their wake the same useless medicines have been tested almost everywhere.
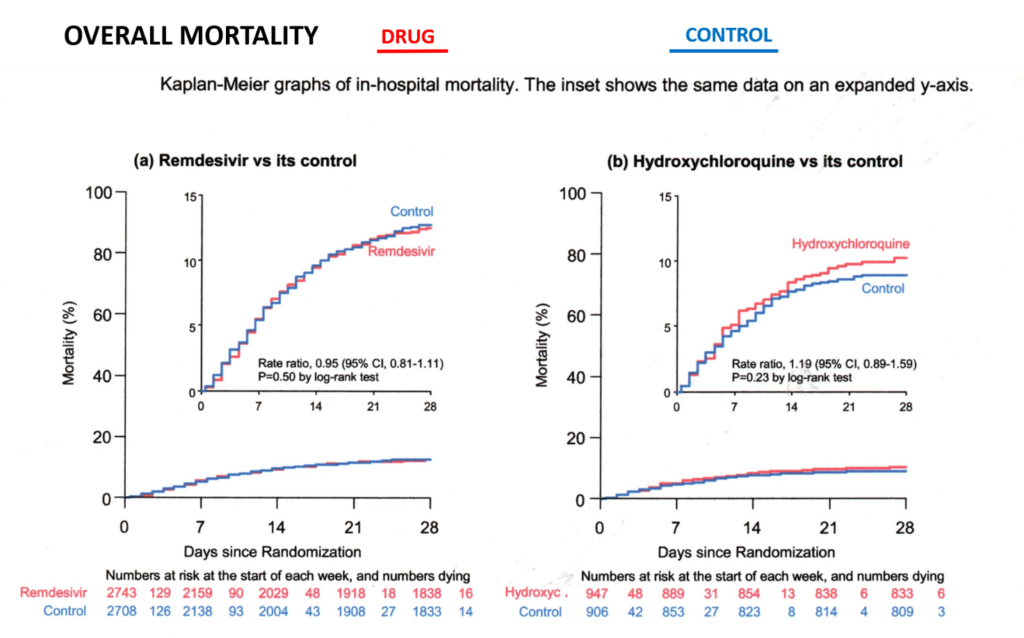
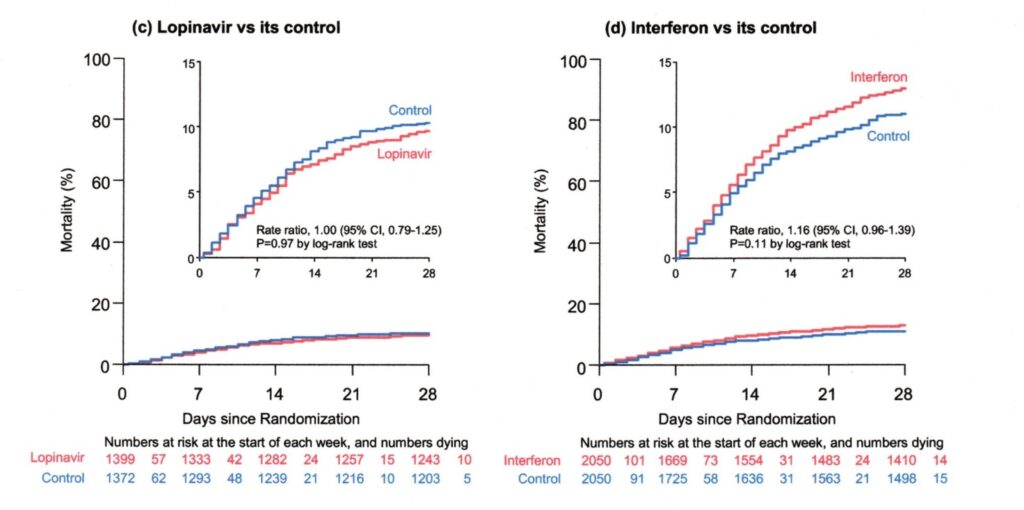
Because they insisted on testing for many months to ascertain whether the therapy was beneficial, which was already evident after a month (statistical elaboration through the Kaplan Meier 28 Day Mortality method, Table 2) (H). In fact mortality was superior to the control group. In these trials mortality for ventilated patients was 41% (Solidarity study), while with the cortisone therapy it was 29% (Recovery Study) (I).All these useless pharmaceutical trials have caused the death of thousands of people under the pretext of scientific research. And all this in general without having requested and obtained the informed consent from the patients/relatives, because a European legal provision exonerated the experimenter from this obligation for the Covid emergency (European Medicines Agency etc.) (J), seriously infringing the fundamental constitutional rights of every citizen. No patient or relative would have signed an informed consent stating that half the patients were left with no treatment but only the placebo.
Because the European governments were advised to authorize the use of Remdesivir on 3 July, (knowing that it was useless) and because they were advised to get huge supplies of this drug (Table 3), which promptly took place (European Commission) (K).
Because a worldwide race for vaccines began, unsafe both for the abbreviated test procedure due to the Covid emergency, but also for the strong economic interests (the over 160 centers in the world have been sponsored on average with 200 Million Euro). There is also hardly any state control of the trials. The sponsor (i.e. who pays for the trials with a high compensation to the hospitals) and the ethical commission are responsible for controlling the correct conduct of the trial itself (the dream of every student: I write the assignment, I mark it and give it a grade). Vaccination during an ongoing epidemic can also trigger serious side effects like the narcolepsy during the vaccination against swine ‘flu in 2009.
In this epidemic too the political reaction proved completely exaggerated. The EU (to name some countries) spent about 1.3 billion in England and over 700 million in France for a vaccine for a ‘flu which had caused only 2,900 deaths in Europe compared to the European average of 40,000 to 220,000 a year from common ‘flu (EC debate 7/3/2011) (L). In 2009 Transparency International (The Global Coalition against Corruption) had already criticized the financing of the European Medicines Agency (EMA) for two thirds of the Pharmaceutical Industry (M). The European Court of Auditors later confirmed this conflict of interest (Press release ECA/12/39 on 11/10/2012) (N).Whoever performs vaccination during an ongoing epidemic commits a graveerror
Because the “VirologicalScience” does not admit to having wrongly assessed the means of transmission of the Coronavirus (O). It is in the same situation as Gottlob Frege (1902), who in the end discovered important errors in his research defining the bases of mathematics (note 3).
Because there is a relentlessness towards children, our future, considering them global super-spreaders.
TRAUMATIZING CHILDREN CONSTITUTES A CRIME AGAINST “HUMANITY”
The answer my friends, is blowing in the wind, the answer is blowing in the wind.
Appendix
Table 1) – Percentage variation in deaths in 2020 compared to the 2015-2019 average, by region, distribution and month.
Report ISTAT, National Institute of Statistics, 22/10/2020
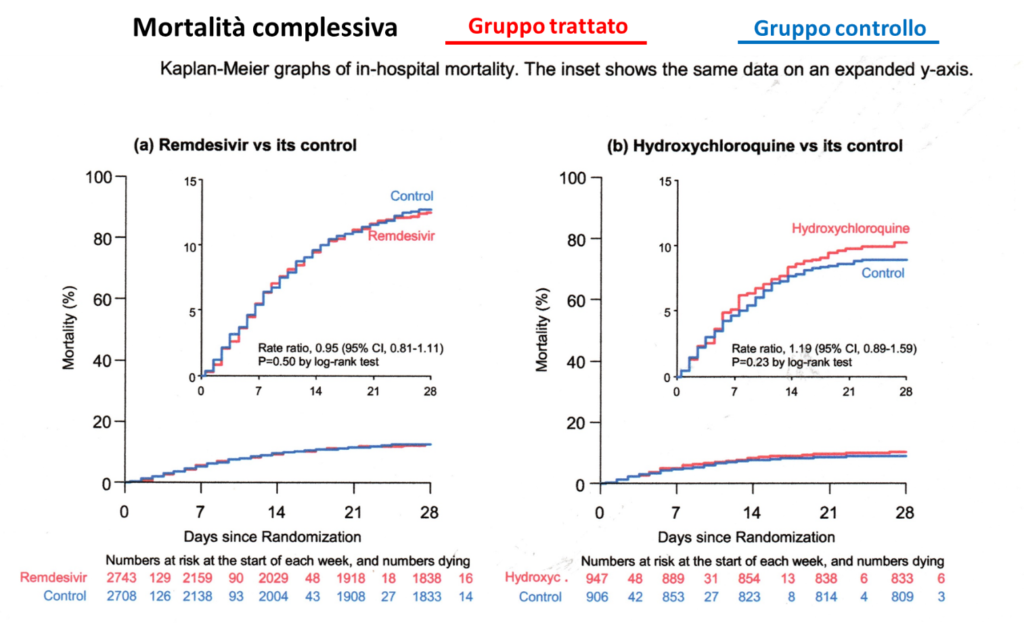
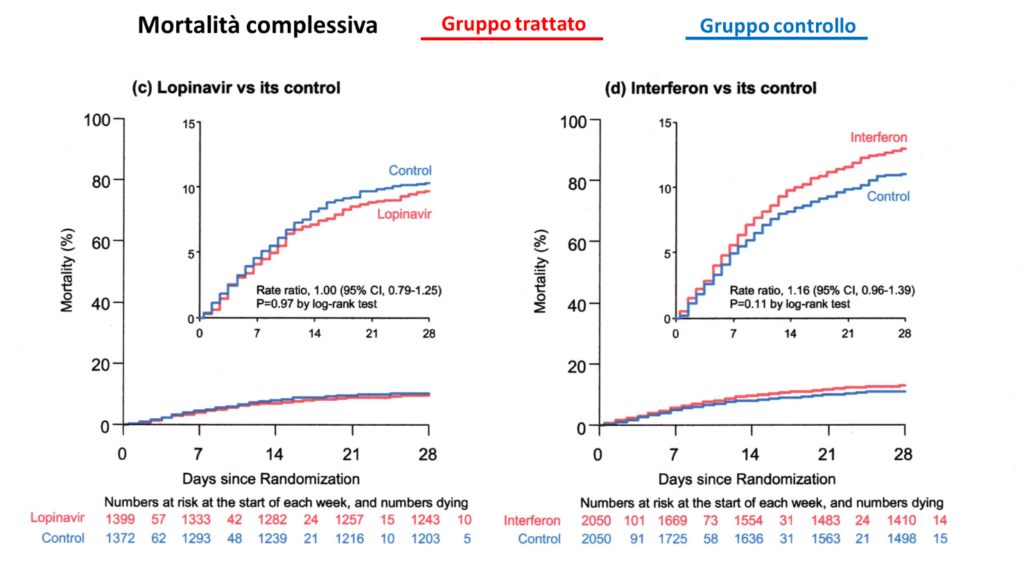
Table 2)
Statistical elaboration: Kaplan Meier 28 day risks (mortality), available monthly from April on the WHO site. The monthly results have clearly shown the inefficacy of the antiviral drugs involved, hence the study should have been interrupted much sooner. Each month of delay causes unnecessary deaths.
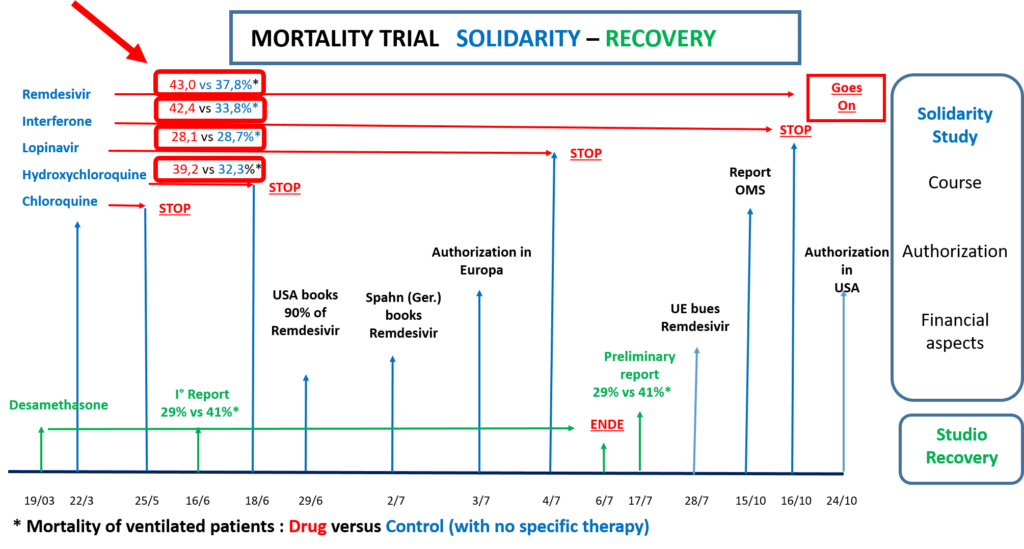
Timeline of the experiments (Mortality PV* = Ventilated Patients, control** = with no specific therapy)
19/03 Recovery trial begins
22/3 Solidarity (S) trial begins monthly report of results
15/10 WHO Report Mortality PV* Remdesivir 43.0%, control** 37.8%
24/10 USA authorizes the use of Remdesivir
Note 1) “National Health Institute, Report n.49/2020, 8/6/2020: “COVID-19: Interim Report on the definition, certification and classification of the causes of death”
According to this report the patients included in the 33.000 until 7/6/20 are composed as follows:
Suspected case (without laboratory investigation: Author’s note)
Someone with acute respiratory infection and with no other etiology, which completely explains the clinical presentation and with a travel or residence history with transmission of the virus.
Someone with any acute respiratory Infection who has been in contact with a probable or confirmed case of Covid.
Probable case: suspected case whose SARS-CoV-2 test result is doubtful or inconclusive (i.e. despite negative test the diagnosis is confirmed: Author’s note)
Confirmed case. Case with laboratory confirmation independently of signs and clinical symptoms.
Note 2) “National Institute of Statistics” ISTAT Report from 16/7/20: “Impact of the Covid-19 epidemic on Mortality: Causes of death of positive deceased from SARS-CoV-2”
The report includes 4,942 statements of death submitted to the National Institute of Health with confirmed SARS-CoV infection. This constitutes only 15.6% of the reported cases until 25/5/20 out of a total of 31.573 deaths. Therefore the remaining cases are suspected or probable cases (i.e.with no laboratory diagnosis).
The statistical elaboration of this small group of patients has emphasised that: “Covid-19 is the directly responsibile cause of death in 89% of deaths of people positive to SARS-CoV-2”, a statement which is repeated daily like a prayer wheel.
Definition of directly responsibile for death: death is caused directly by Covid-19, when death would not have been verified, if the SARS-Cov-2 infection had not intervened (although often overlapping other pre-existing illnesses and their complications).
Note 3) The virological community should publicly release the same declaration as Frege on 16/6/1902 (modified by vaso di pandora): “Hardly anything more unwelcome can befall a scientific writer (virological community) than that one of the foundations of his edifice be shaken after the work (program for the “fight” against the pandemic) is finished. This is the position into which I was put (still Frege) by a letter from Mr Betrand Russell (Wegener der Weltbildzertruemmerer), as the printing of this volume (Public Measures against the Pandemic) was nearing completion.
Ministero della Salute Italiano: Covid-19: Situazione in Italia al 4/11/2020. http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?area=nuovoCoronavirus&id
D) Istituto Superiore della Sanità (ISS): COVID-19: rapporto ad interim su definizione, certificazione e classificazione delle cause di morte, n.49/2020. 8/6/20
E) Istituto di Statistica Italiana: Impatto dell’epidemia COVID-19 sulla mortalità: cause di morte nei deceduti positivi a SARS-COV-2, https://www.istat.it/it/archivio/245573
CETERUM CENSEO, CARTAGINEM ESSE DELENDAM, così finiva Catone, il Censore, ogni suo intervento al senato.
In tale senso: Ceterum Censeo, che la situazione non è di natura medica ma di natura politica/economica, il bene e la salute pubblica non c’entra niente, le persone comuni non sono altro che carne da cannone:
Curva -Giallo : attualmente positivi, Verde: guariti, Grigio: decessi
Perché avviene giornalmente una disinformazione organizzata della popolazione riguardante mortalità, letalità, indice di contagiosità, deceduti, infetti nuovi, reinfezione, asintomatici, portatori sani, positivi. Quest’ultimi vengono inseguiti con tutti i mezzi a disposizione dello stato, come se fossero dei delinquenti. Ma questa caccia non ha senso, essendo l’indice di contagiosità completamente scollegato dalla mortalità, come evidenziato dalla statistica emessa dal governo italiano il 4/11/20 (A).
Perché vengono diffuse ogni giorno notizie disastrose per quanto riguarda la pandemia, nonostante che in questo anno (Italia come esempio, in Germania non sono disponibili i dati a tale proposito) non c’è stato un aumento statisticamente significativo della mortalità rispetto al periodo 2015-2019. Nel periodo maggio-agosto ci fu addirittura una riduzione della mortalità rispetto ai cinque anni precedenti del 1.6% (Report ISTAT, Istituto Nazionale di Statistica, 22/10/2020 (Tabella 1)(B).
Perché le statistiche diffuse dalle media prevedono un aumento considerevole dei decessi da coronavirus con previsioni angoscianti per il futuro, (“fra poco più di 1000 morti al giorno”), nonostante la letalità da Coronavirus viene stimato del 0.14% contro il 0.10 della influenza comune (WHO 14/10/20)(C). Questo forse perché pazienti anche senza conferma di laboratorio, vengono inclusi nella mortalità con la sola diagnosi di sospetto (a causa di valutazione medica o epidemilogica) (Rapporto del Istituto Superiore della Sanità (ISS), n.49/2020,8/6/20, nota 1)(D), oppure perché la elaborazione statistica fu eseguita su gruppi limitati di pazienti (4942 di 31.573 morti per Coronavirus al 25/05/2020), oppure perché sono stati utilizzati termini di definizioni inadatte. Sotto il termine “direttamente responsabile per il decesso”, si intende, che il decesso non si sarebbe verificato se l’infezione da SARS-CoV-2 non fosse intervenuta, seppure spesso sovrapposto ad altre malattie preesistenti, e dalle sue complicanze (Report del “Istituto Nazionale di Statistica” ISTAT) del16/7/2020: Impatto dell’epidemia Covid-19 sulla mortalità: Cause di morte dei positivi a SARS-CoV-2, nota 2)(E).
Attualmente quasi tutti i ospedali in quasi tutto l’Europa sono pressoché pieni di pazienti di Coronavirus, nonostante la mortalità attuale è molto inferiore rispetto alla primavera. Inoltre nel frattempo fu aumentata la capacità dei letti ospedalieri per pazienti da Coronavirus,. Potrebbe servire questo, per recuperare il deficit dei ospedali causato dalla drammatica riduzione dei accessi ai ospedali a causa della pandemia (il deficit nei primi 4 mesi in Italia è di 3.5: Report ALTEMS Alta Scuola di Economia e Management dei sistemi Sanitari) (F). In tale maniera si può raggiungere il Budget, per non rimanere insolvente (“Coronavirus rettet die Kliniken, aber die Pleitegefahr bleibt hoch” = la crisi da coronavirus salva gli ospedali, ma il rischio di fallimento rimane alto. Das Handelsblatt ) (G). In Germania lo stato paga ai ospedali circa 700 euro per ogni letto non occupato con la motivazione, di tenerlo libero per l’attesa della eventuale seconda onda della pandemia. Tutto questo perché sovvenzioni diretti a livello della Communita europea non sono più permessi. Se qualcuno non può rispettare i suoi obblighi finanziari, deve dichiarare insolvenza, un disastro per la sanità pubblica.
Perché venivano autorizzate a marzo sperimentazioni a largo spettro a livello mondiale di farmaci antivirali quali Remdesivir (Solodarity ecc.) con il gruppo di controllo, che non otteneva nessuna terapia farmacologica specifica, che invece doveva essere il cortisone. Nella loro scia sono state sperimentate quasi ovunque le stesse medicine inutili.
Perché si insisteva nella sperimentazione per molti mesi per appurare che la terapia aveva alcun beneficio, il che era già evidente dopo un mese (elaborazione statistica tramite metodo Kaplan Meier 28 Day Mortality, Tabella 2) (H). Anzi la mortalità era addirittura superiore al gruppo di controllo. La mortalità in questi studi per pazienti ventilati era del 41% (studio Solidarity), mentre quella con la terapia con cortisone era del 29% (Studio Recovery) (I).Tutte queste sperimentazioni farmaceutiche inutili hanno causato la morte di migliaia di persone con il pretesto della ricerca scientifica. E tutto questo in linea di massima senza aver chiesto ed ottenuto il consenso informato da parte dei pazienti/parenti, perché un a disposizione legge in Europa esonerava per l’emergenza Covid lo sperimentatore da questo obbligo (European Medicines Agency ecc.) (J), ledendo in maniera grave i diritti costituzionali fondamentali di ogni cittadino. Nessuno paziente oppure parente avrebbe firmato un consenso informato contenente l’affermazione, che la metà dei malati venivano lasciati senza terapia di riferimento ma solo con il placebo.
Perché fu consigliato ai governi europei di autorizzare l’utilizzo del Remdesivir il 3 Luglio, (sapendo che era inutile e perché fu consigliato a loro di fare approvvigionamenti ingenti di tale farmaco (Tabella 3),.come prontamente avvenuto (European Commission) (K).
Perché fu iniziata una corsa ai vaccini in tutto il mondo, insicuro sia per la procedura di sperimentazione abbreviata a causa della emergenza Covid, ma pure per i forti interessi economici (i oltre 160 centri nel mondo sono sponsorizzati mediamente con 200 Milione di Euro). Inoltre manca pressoché completamente un controllo statale dei studi. Lo sponsor (cioè chi paga la sperimentazione con un forte compenso ai ospedali) e la commissione etica sono i responsabili per controllare il corretto svolgimento della sperimentazione stessa (il sogno di ognun studente: io scrivo il compito, il lo correggo ed io do il voto). Inoltre la vaccinazione durante una epidemia in corso può comportare dei seri effetti collaterali come la narcolessia durante la vaccinazione contro l’influenza suina del 2009. Anche in questa epidemia la reazione politica si era dimostrato completamento esagerata. Sono stati spesi dall’Unione Europea (per nominare alcuni paesi) circa 1.3 miliardi in Inghilterra e oltre 700 milioni in Francia per il vaccino per una influenza, che aveva causato in Europa solo 2900 decessi rispetto alla media in Europa della influenza comune di 40.000 a 220.000 l’anno (dibattito Comunione Europea del 7/3/2011) (L). Trasparency International (The Global Coalition against Corruption) aveva già nel 2009 criticato il finanziamento della Agenzia Europea del Farmaco (EMA) per i due terzi dalla Industria Farmaceutica (M). In seguito la Corte dei Conti Europea ha confermato questo conflitto d’interesse (Comunicazione stampa ECA/12/39 del 11/10/2012) (N).Chi effettua una vaccinazione durante una epidemia in corso commette un grave errore
Perché la “Scienza Virologica” non ammette, di aver valutato in maniera sbagliata la via di trasmissione del Coronavirus (O). Essa trova nella stessa situazione come Gottlob Frege (1902), che nella sua ricerca, di definire le basi della matematica, alla fine ha riscontrato dei errori importanti (nota 3).
Perché c’è un accanimento contro i bambini, il nostro futuro, considerandoli untori del mondo (lavori dei bambini).
TRAUMATIZZARE I BAMBINI COSTITUISCE UN CRIMINE CONTRO L‘UMANITA’
The answer my friends, is blowing in the wind, the answer is blowing in the wind.
Appendice
Tabella 1)
Report ISTAT, Istituto Nazionale di Statistica, 22/10/2020
Tabella 2)
Elaborazione statistica: Kaplan Meier 28 day risks (mortality), da aprile mensilmente consultabile presso il sito OMS. I risultati mensilmente hanno chiaramente dimostrato l’inefficacia dei farmaci antivirali impegnati, per cui lo studio doveva essere interrotto molto prima. Ogni mese di ritardo è causa di decessi evitabili.
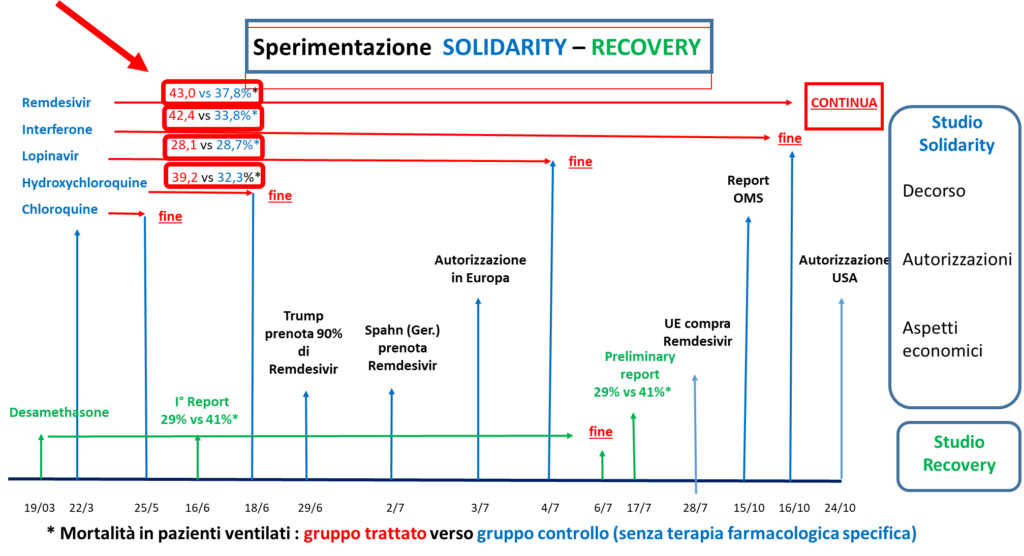
Tabella 3)
Cronologia delle sperimentazioni (Mortalità PV* = Pazienti Ventilati, controllo** = senza terapia specifica)
Cronologia delle sperimentazioni: Gruppo trattato, gruppo controllo (senza terapia farmacologica specifica), mortalità di pazienti ventilati in %
19/03 Inizio trial Recovery Cortisone
22/3 Inizio trial Solidarity (S) Chloroquine, Hydroxychloroquine, Lopinavir, Interferone, Remdesivir
25/5 Chloroquine esce da Solidarity
16/6 I° Report Recovery Cortisone: 29%, controllo : 41%
18/6 Hydroxychloroquine esce da Solidarity
H.chloroquine : 39.2%, controllo : 32.3%
29/6 USA prenotano 90% delle risorse Remdesivir
2/7 Germania prenota Remdesivir
3/7 Autorizzazione Unione Europea (UE)
4/7 Lopinavir esce da Solidarity
Lopinavir : 28.1%, controllo 28.7%
6/7 Fine trial Recovery
17/7 Report trial Recovery Cortisone : 29%, controllo : 41%
28/7 UE compra Remdesivir
15/10 Report WHO Remdesivir : 43.0%, controllo : 37.8%
16/10 Interferone esce da Solidarity
Interferone : 42.4%, controllo : 33.8%
24/10 Autorizzazione USA
Nota 1) Report dell’”Istituto Superiore della Sanità, n.49/2020, 8/6/2020: “COVID-19: Rapporto ad interim su definizione, certificazione e classificazione delle cause di morte”
Secondo questo rapporto i pazienti inclusi nei 33.000 fino al 7/6/20 si compongono come segue:
Caso sospetto (senza indagine di laboratorio: Nota dell’autore) :
Persona con infezione respiratoria acuta e senza un’altra eziologia, che spieghi completamente la presentazione clinica e con storia di viaggi o residenza con trasmissione del virus.
Persona con qualsiasi infezione respiratoria acuta che è stato in contatto con caso probabile o confermato Covid.
Caso probabile: caso sospetto il cui risultato al test per SARS-CoV-2 è dubbio o inconcludente (cioè nonostante test negativo viene confermato la diagnosi: Nota dell’autore)
Caso confermato. Caso con conferma di laboratorio indipendentemente dai segni e dai sintomi clinici.
Nota 2) Report dell’”Istituto Nazionale di Statistica” ISTAT del 16/7/20: “Impatto dell’epidemia Covid-19 sulla Mortalità: Causa di morte dei deceduti positivi al SARS-CoV-2”
Il rapporto include 4942 schede di morte pervenute all’ Istituto superiore della Sanità con infezione da SARS-CoV confermati. Questo costituisce solo il 15.6% dei casi segnalati fino al 25/5/20 su un totale di 31.573 deceduti. Il rimanenti casi sono allora casi sospetti o probabili (cioè senza diagnosi di laboratorio.)
La elaborazione statistica di questo esiguo gruppo di paziente ha evidenziato che: “Covid-19 è la causa direttamente responsabile della morte nell’89% dei decessi di persone positive al SARS-CoV-2”, una affermazione, che viene giornalmente ripetuta come una ruota della preghiera.
Definizione direttamente responsabile per la morte: la morte è causata direttamente da Covid-19, quando il decesso non si sarebbe verificato, se l’infezione da SARS-Cov-2 non fosse intervenuta (seppure spesso sovrapposto ad altre malattie preesistenti e delle sue complicanze).
Nota 3) La comunità virologica dovrebbe rilasciare pubblicamente la stessa dichiarazione come Frege il 16/6/1902 (modificato da vaso di pandora): Ad un autore scientifico (comunità virologica) difficilmente puo accadere una cosa piu indesiderata dopo la il completamento della sua opera (programma per la “lotta” contro la pandemia), che una base della sua costruzione viene scosso. In questa situazione mi sono trovato (sempre Frege) a causa della lettera del Sig. Bertrand Russell (Wegener der Weltbildzertruemmerer), quando la stampa del mio libro (Misure Pubblichecontro la Pandemia) giungeva alla fine.
D) Istituto Superiore della Sanità (ISS): COVID-19: rapporto ad interim su definizione, certificazione e classificazione delle cause di morte, n.49/2020. 8/6/20
E) Istituto di Statistica Italiana: Impatto dell’epidemia COVID-19 sulla mortalità: cause di morte nei deceduti positivi a SARS-COV-2, https://www.istat.it/it/archivio/245573
The aerosol as the only significant mode of transmission of the coronavirus: epidemiological evidence
Introduction: There are currently many different opinions, partly contrasting with regard to the transmission of coronavirus and the measures to be taken to deal with it. At present the main mode of transmission is considered to be through droplets or contact. The aim of this article is to examine the importance of transmission through contact and droplets against transmission by aerosols using an epidemiological approach. To this end three regions of Italy have been compared as cohorts.
Material and Methods: The three regions included in this study are Lombardy, Emilia Romagna and Sicily. A clinical analytical study has been carried out on these three cohorts. The relative homogeneity at the beginning of the epidemic (general risk of exposure, demographic conditions) and eventual interaction during the observation period have been assessed. 24/04/2020 was considered the final date of the survey in relation to fatal cases.
The results were assessed with regard to transmission through contact/droplets or by aerosols.
Results:
Lombardy, Emilia Romagna and Sicily are fairly similar as regards territorial extent (Lombardy: 23,865 km2,, Emilia Romagna 22,453 and Sicily 25,832 km2) As for population/population density per km2, Emilia Romagna and Sicily are comparable (Emilia Romagna 4,459,477/198.6 per km 2, Sicilia 4,999,891/193.6 per km 2). Lombardy has an approximately double population/population density (10,060,574/421.6 per km2).
The homogeneity of the two cohorts in the north as regards risk of exposure is comparable due to the similar geographical, demographic and climatic conditions. Sicily, 1000 kilometers further south, until the end of March was exposed to a similar if not much higher exposure:
Catania airport (metropolis with over a million inhabitants) took 6th place in Italy last year for passenger transport, in Germany it would be little after Stuttgart, Cologne and Berlin Tegel at 9th place. Compared to the previous year, air traffic in Catania in January increased by 4.94% to 609,750 and in February by 1.36% to 547,210: Lombardy is in third place overall for presences in Sicily (1,069,293) after France (1,584,410) and Germany (1,185,041)
From 3 to 5 February the Festival of St Agatha took place, one of the largest religious festivals in the world with a turnout of over a million people, obviously with no social distancing.
After the closure of universities, bars, restaurants etc. there was a justified return of students and workers from the north: around 40,000 people who registered spontaneously (Note from the Ministry 24/03/20), even if the actual figures will be considerably higher.
Until International Women’s Day (8 March) as regards the winter season, Catania was the city in Italy and Europe with the highest quota of social personal contacts due to the very intense daily and night life. This was caused by the extensive presence of people both from outside and inside the territory. In this period Catania pulsated from early morning until long after midnight.
As for the homogeneity of the cohorts regarding healthcare and political interference, no differences were found. (The various government decrees applied to the whole of Italy).
26 April 2020 was taken as the final point of the study. According to government statistics the following data were recorded for the number of deaths:
Discussion: three Italian regions were included in this study, two from the north: Lombardy and Emilia Romagna and Sicily 1000 km further south. The structure of the population is similar with the exception of Lombardy which has double the density of the other two regions. The starting point of the epidemic (end of January, beginning of February) is comparable as regards risk of exposure (possibly higher in Sicily). The lockdown ordered by the government meant that the course of the epidemic was not altered by regional interaction. This allows a homogeneity of the cohorts virtually unique in medicine.
The evaluation of the results regarding the two factors considered responsible for transmission (droplets/aerosols) leads to the following conclusions:
The importance of transmission through contact, droplets etc. in relation to the course of the epidemic goes towards zero. This is evident from the fact that the necessary interpersonal contact is similar in the three cohorts (certainly much higher in Sicily, especially in big cities), but the death toll in Sicily is very low. (Sanitary conditions, often considered to be the cause of this mode of transmission, are similar in North and South Italy).
The importance of transmission by aerosols remains the only determining factor. The explanation lies in the analysis of the differing living conditions in the home-work environment between the north and the south. Staying in the open air and in insufficiently ventilated environments are identified as determining factors.
The habitat of the Sicilian population, due to the climatic and industrial conditions, is fundamentally different to that in the North.
Buildings are not insulated to guarantee energy efficiency (the concentration of CO2 is an indicator for risk of infection: Rudnick and Milton 2003), they have high ceilings to provide coolness in the summer.
Heating is only used to a limited extent (both in private and public spaces) and there is also sufficient ventilation (see the indications for a healthy climate in buildings) in winter facilitated by the relative difference between the external and internal temperature.
Life in Sicily takes place outside to a great extent also in winter thanks to the mild climate.
Industrial plants with a high concentration of people are far less common than in the North.
There is adequate ventilation in means of transport (cars, buses, trains).
As transmission by aerosols finds an ideal situation in the closed environments in northern Italy (the concentration of CO2 will be caused by the high level of insufficient ventilation) we are faced with, in the broad sense, the already well known Sick building Syndrome (Finnegan et al. 1984). .
The theory of transmission by aerosols is also confirmed in the virological literature. Particles the size of the coronavirus settle at the level of the lower respiratory tract (Bottarelli 2020). The involvement of the oropharyngeal cavity and the upper respiratory tract are to be considered secondary, occurring following exhaled air, not significant for transmission.
Conclusions: As transmission, as explained above, occurs by aerosols (influenza too, showing the same epidemiological features as the coronavirus, probably follows the same mode of transmission) the measures currently being taken (quarantine/lockdown, masks, gloves, measures against gatherings) should be corrected immediately.
It is vitally and urgently important to undertake measures to rectify the human habitat regarding both internal and external pollution.
Bibliography (in limited edition due to the coronavirus)
Finnegan MJ, Pickering CA, Burge PS: The sick building Syndrome: Prevalence Studies. Br Med J. 1984; 289:1573-5