The four elimination pathways and Coronavirus or:
Medicine is not a science but an opinion.
The obligation for masks is considered one of the most effective measures to combat the coronavirus pandemic. This measure is imposed, like many others, only for populist political reasons and is not only completely ineffective with regard to a reduction in the transmission of the virus, but also constitutes a serious danger to the health of anyone wearing the mask (1) (European Centre for Disease Prevention and Control 2020). This problem is sidetracked, deliberately creating great confusion among the sick, the dead, the HIV-positive, the healthy carriers, the asymptomatic, the positive etc.
In the end the contagiousness index was introduced (Robert Koch Institute) as the supreme judge of good and evil, which arbitrarily divides countries into zones of good and bad citizens, the latter to be ruthlessly punished. All this happens with no scientific basis and is statistically unacceptable, but the hunt for positives with all available means (immune App etc.) has become one of the “main weapons in the fight against the Coronavirus”. Those discovered positive and their families are put under house arrest and pilloried, as if they were criminals.
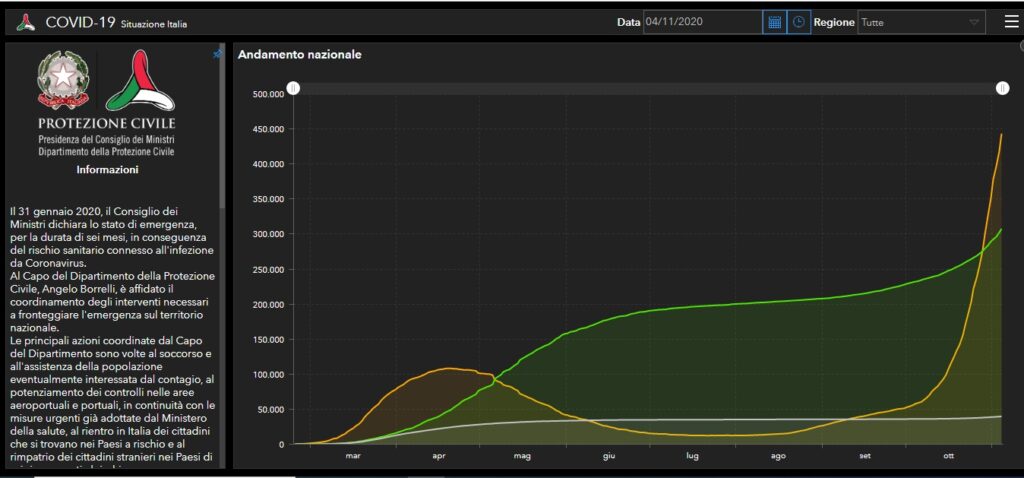
But this hunt makes no sense, as the contagiousness index is completely unrelated to mortality, as shown by the statistics issued by the Italian Ministry of Health/ Ministero della Salute Italiano on 4/11/20 (2).
BUT WHAT IS WRONG WITH MASKS?
I’ll explain it in a nutshell.
Our body has four elimination pathways for noxious substances: urinary tract (urine), digestive tract (feces), skin (perspiration) and the lungs (respiration). This last pathway, important with regard to coronavirus transmission, must guarantee both the oxygen/carbon dioxide exchange and the ventilation of the respiratory tracts, the nasal and paranasal sinuses and the middle ear.
If this or any other pathway is interrupted or reduced, the body gets progressively intoxicated and damaged even irreversibly.
And now we come to masks:
- Masks in no way protect against coronavirus infection as the means of transmission is exclusively aerial by aerosols (3) and not through droplets or contact.
The Coronaviruses have a superimposable shape to that of various pollens (one of nature’s wonders) but they are much smaller and are transmitted in the same way, suspended and transported by air. If they land on fertile ground (for the coronavirus the peripheral airways, i.e. the bronchioles) they take root and then multiply.
Their dimensions are also comparable to those of smoke particles, they get to the alveoli and are then inhaled and exhaled. This is the difference to droplet particles, which having a diameter about 60 times higher, are picked up by the upper respiratory tracts.

The Coronavirus’ gateway to the body and its replication finally take place at the level of the peripheral airways (bronchioles), where they induce an inflammatory response mediated by antibodies similar to allergic asthma. This is why the severity of the disease does not primarily depend on the damage caused to the organism by the virus, but on the damage caused by the immune system to the organism (4), which is why cortisone was the first choice drug in aggravated cases at the beginning of the pandemic.
The modes of falling ill with coronavirus are comparable to those of falling ill from passive smoking. Coming into contact with people who transmit coronavirus is the same as coming into contact with smokers. The harmful agent is inhaled in the same way and the dangerous load for the organism only takes place in closed, badly ventilated environments.
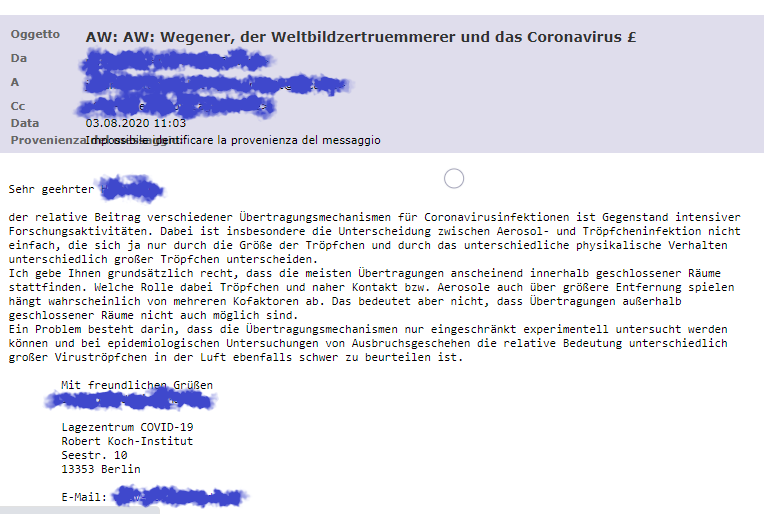
In this respect the Robert Koch Institute has confirmed that transmission of the virus in the open is highly improbable (RKI).
- Masks are very dangerous because they greatly reduce the aeration of the lungs.
Once respiratory system patients were sent to the mountains or the sea to exhale the unhealthy air and inhale clean air, whereas now they are provided with masks and the exhaled air (which contains a high number of viruses during the infectious phase) cannot disperse in the open air but is retained by the mask and subsequently inhaled.

In this respect masks oblige people to infect themselves more and more (as if one smoked under the mask), condemning them to an increasingly serious risk to their health and producing severely ill patients.
And so, breath by breath, people reduce their chances of survival. HOORAY FOR MEDICINE!
Unfortunately medicine is not a science, but an opinion. Day by day many opinions (political, economic, populist etc.) interfere on the orientation of medicine, also with compliant experts in the medical sphere. In arithmetic, (which is a science) one and one makes two (1+1=2), in medicine (which is an opinion) 1+1 does not always make 2, it eventually makes 3, 4 or 18, 24, maybe better 42-2, according to the current opinion.

With the current government measures we are actually forced to take refuge in closed places, right where we get infected and then we are forced to endure serious or very serious harm caused by the obligation for masks. We are taken right there, young and old, where we don’t want to end up, in the arms of the angel of death.

APPENDIX:
Ceterum censeo, Cartaginem esse delendam, thus Cato, the Censor finished each of his speeches at the Senate.
In this sense this contribution ends with: Ceterum Censeo, that the situation is not of a medical but a political/economic nature, public good and health have nothing to do with it, common people are nothing but cannon fodder:
- Because there is a daily organized disinformation of the population regarding mortality, lethality, contagiousness index, deceased, newly infected, re-infection, asymptomatic, healthy carriers, positives. The latter are pursued with all the means at the disposal of the state, as if they were criminals. But this hunt makes no sense, as the contagiousness index is completely unrelated to mortality, as shown by the statistics issued by the Italian government on 4/11/20 (A).
- Because disastrous news is broadcast every day regarding the pandemic, even though this year (e.g. in Italy, in Germany the relevant data is not available) there has not been a statistically significant rise in mortality compared to the period 2015-2019. From May-August there was even a reduction in mortality compared to the five previous years by 1.6% (ISTAT Report, National Institute of Statistics 22/10/2020 (Table 1)(B).
- Because the statistics released by the media predict a significant increase in deaths from coronavirus with distressing forecasts for the future, (“soon over 1,000 deaths a day”), even though the lethality of Coronavirus is estimated at 0.14% against the 0.10 of common ‘flu (WHO 14/10/20)(C). Possibly because even patients without laboratory confirmation are included in the deaths with only a suspected diagnosis (as a result of medical or epidemiological evaluation) (Report of the National Health Insitute (ISS), n.49/2020,8/6/20, note 1)(D), or because the statistical elaboration was carried out on limited groups of patients (4942 of 31.573 deaths from Coronavirus to 25/05/2020), or because inappropriate terms of definition were used. The term “directly responsible for death”, means that the death would not have beenverified if the SARS-CoV-2 infection had not intervened, although often overlapping other pre-existing conditions, and their complications. (Report from the “National Institute of Statistics on16/7/2020: Impact of the Covid-19 epidemic on mortality: Causes of death of SARS-CoV-2 positives, note 2)(E).
- At the moment almost all the hospitals in almost all Europe are nearly full of Coronavirus patients, even though current mortality is much lower than in the spring. Also the capacity of hospital beds for coronavirus patients has increased since then. This could serve to recover the deficit of hospitals caused by the dramatic reduction in hospital admissions due to the pandemic (the deficit in the first 4 months in Italy is 3.5 bilions of Euro: Report ALTEMS) (F). In this way the Budget can be met, so as not to remain insolvent. (“Coronavirus rettet die Kliniken, aber die Pleitegefahr bleibt hoch” = the coronavirus crisis saves the hospitals, but the risk of bankruptcy remains high. Das Handelsblatt ) (G). In Germany the state pays the hospitals about 700 euro for every unoccupied bed, to keep it free for the eventual second wave of the pandemic. All this because direct subsidies at EU level are no longer permitted. If someone cannot uphold their financial obligations, they have to declare insolvency, a disaster for public healthcare.
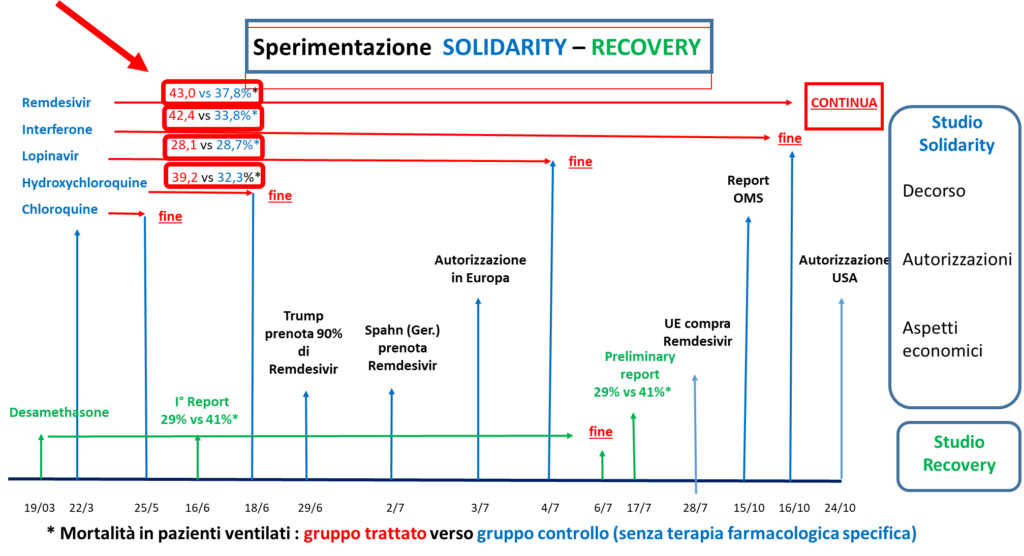
- Because in March wide-spectrum trials of antiviral drugs like Remdesivir (Solodarity etc.) were authorized globally, where the control group did not receive any specific pharmacological drug, which actually should have been cortisone. In their wake the same useless medicines have been tested almost everywhere.
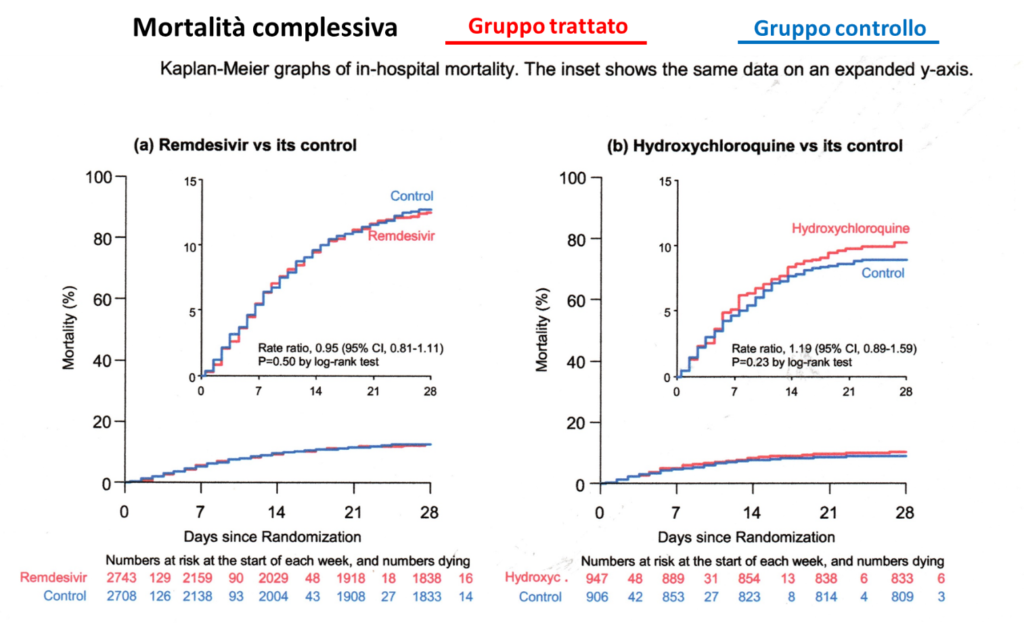
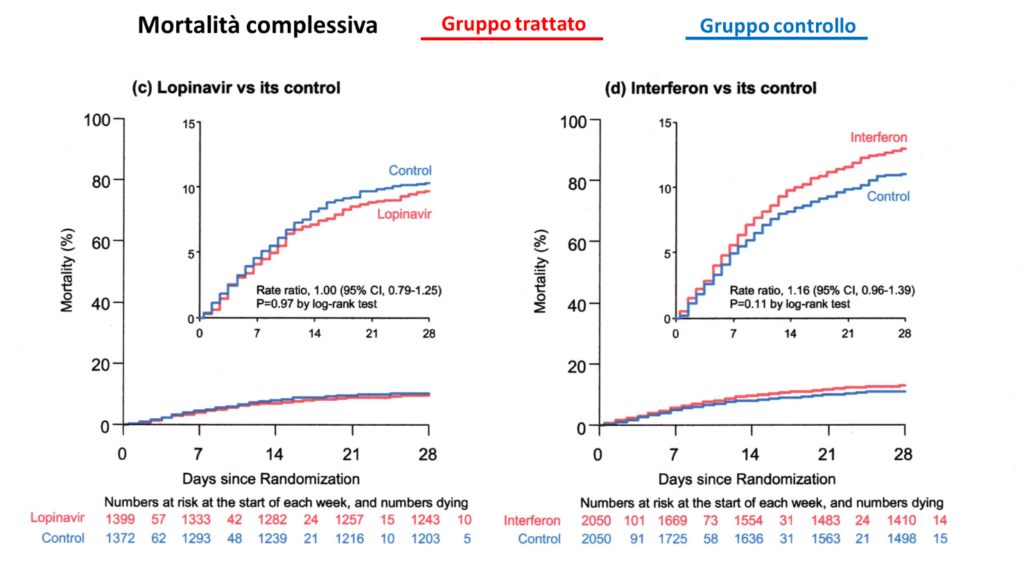
- Because they insisted on testing for many months to ascertain whether the therapy was beneficial, which was already evident after a month (statistical elaboration through the Kaplan Meier 28 Day Mortality method, Table 2) (H). In fact mortality was superior to the control group. In these trials mortality for ventilated patients was 41% (Solidarity study), while with the cortisone therapy it was 29% (Recovery Study) (I). All these useless pharmaceutical trials have caused the death of thousands of people under the pretext of scientific research. And all this in general without having requested and obtained the informed consent from the patients/relatives, because a European legal provision exonerated the experimenter from this obligation for the Covid emergency (European Medicines Agency etc.) (J), seriously infringing the fundamental constitutional rights of every citizen. No patient or relative would have signed an informed consent stating that half the patients were left with no treatment but only the placebo.
- Because the European governments were advised to authorize the use of Remdesivir on 3 July, (knowing that it was useless) and because they were advised to get huge supplies of this drug (Table 3), which promptly took place (European Commission) (K).
- Because a worldwide race for vaccines began, unsafe both for the abbreviated test procedure due to the Covid emergency, but also for the strong economic interests (the over 160 centers in the world have been sponsored on average with 200 Million Euro). There is also hardly any state control of the trials. The sponsor (i.e. who pays for the trials with a high compensation to the hospitals) and the ethical commission are responsible for controlling the correct conduct of the trial itself (the dream of every student: I write the assignment, I mark it and give it a grade). Vaccination during an ongoing epidemic can also trigger serious side effects like the narcolepsy during the vaccination against swine ‘flu in 2009.
- In this epidemic too the political reaction proved completely exaggerated. The EU (to name some countries) spent about 1.3 billion in England and over 700 million in France for a vaccine for a ‘flu which had caused only 2,900 deaths in Europe compared to the European average of 40,000 to 220,000 a year from common ‘flu (EC debate 7/3/2011) (L). In 2009 Transparency International (The Global Coalition against Corruption) had already criticized the financing of the European Medicines Agency (EMA) for two thirds of the Pharmaceutical Industry (M). The European Court of Auditors later confirmed this conflict of interest (Press release ECA/12/39 on 11/10/2012) (N).Whoever performs vaccination during an ongoing epidemic commits a grave error
- Because the “VirologicalScience” does not admit to having wrongly assessed the means of transmission of the Coronavirus (O). It is in the same situation as Gottlob Frege (1902), who in the end discovered important errors in his research defining the bases of mathematics (note 3).
- Because there is a relentlessness towards children, our future, considering them global super-spreaders.
TRAUMATIZING CHILDREN CONSTITUTES A CRIME AGAINST “HUMANITY”

The answer my friends, is blowing in the wind, the answer is blowing in the wind.
Appendix
Table 1) – Percentage variation in deaths in 2020 compared to the 2015-2019 average, by region, distribution and month.
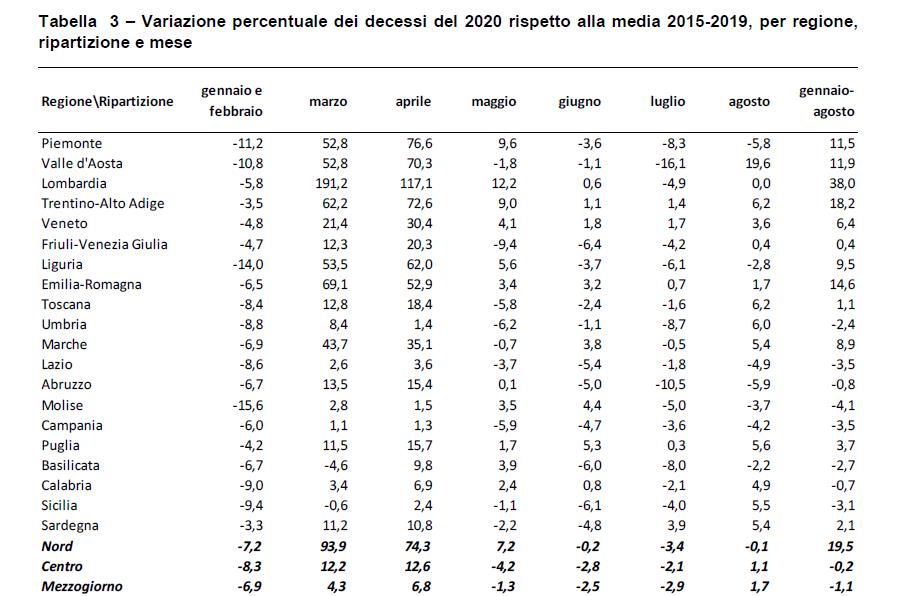
Table 2)
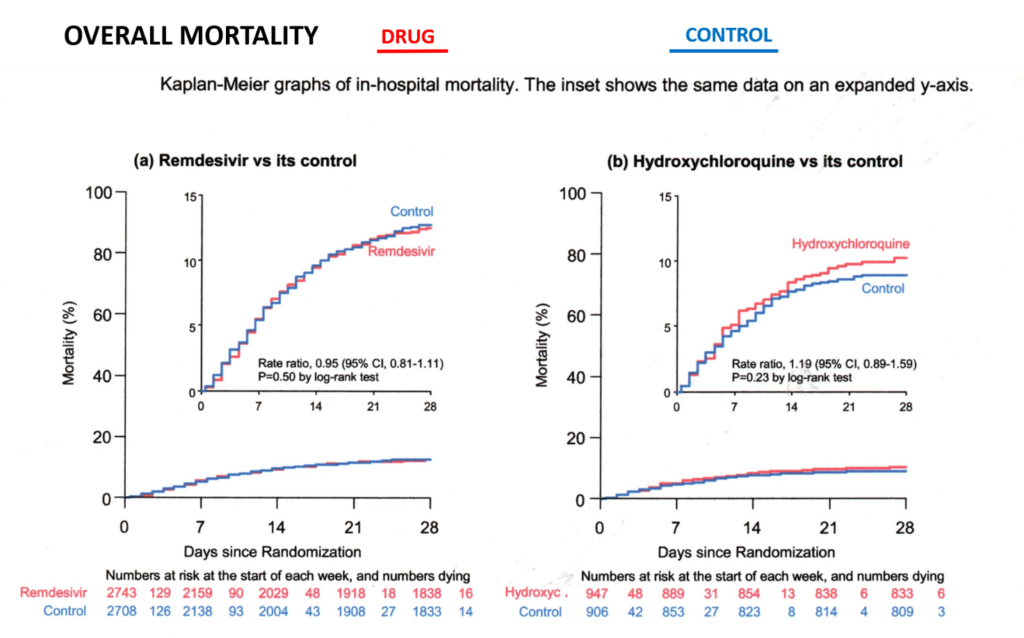
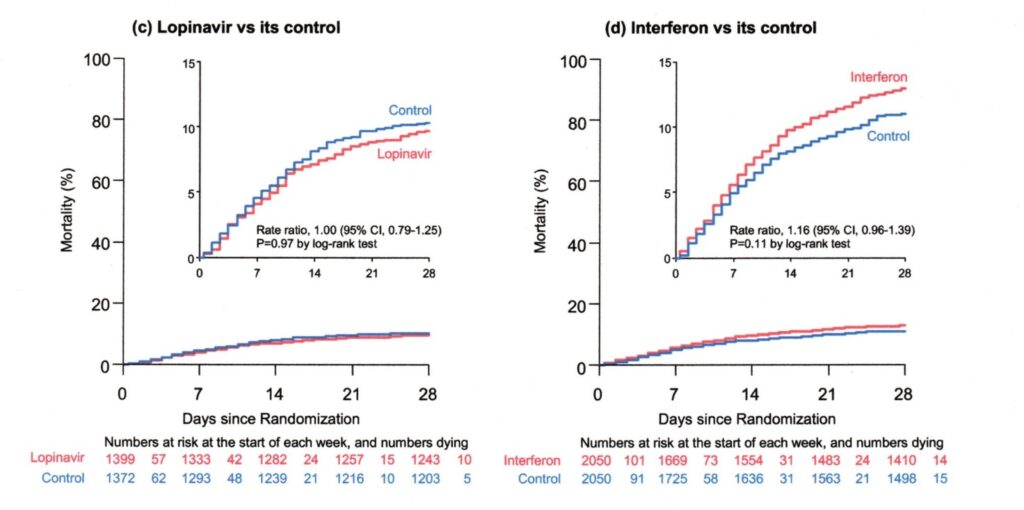
Statistical elaboration: Kaplan Meier 28 day risks (mortality), available monthly from April on the WHO site. The monthly results have clearly shown the inefficacy of the antiviral drugs involved, hence the study should have been interrupted much sooner. Each month of delay causes unnecessary deaths.
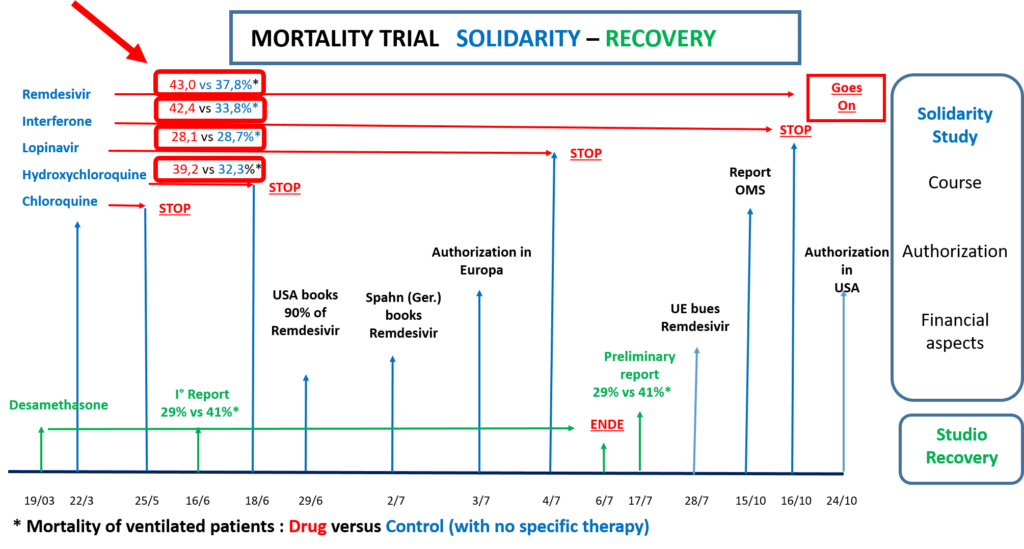
19/03 Recovery trial begins
22/3 Solidarity (S) trial begins monthly report of results
25/5 Chloroquine leaves Solidarity
16/6 1st Recovery Report Mortality PV* Cortisone: 29%, control** 41%
18/6 Hydroxychloroquine leaves Solidarity: Mortality PV* H.chloroquine 39.2%, control** 32.3%
29/6 USA books 90% of the Remdesivir resources
2/7 Germany (Spahn) books large reserves of Remdesivir
3/7 UE authorizes the use of Remdesivir
4/7 Lopinavir leaves Solidarity Mortality PV* Lopinavir 28.1%, control** 28.7%
6/7 Recovery trial ends
17/7 Recovery trial Report Mortality PV* Cortisone 29%, control** 41%
28/7 UE buys Remdesivir
15/10 WHO Report Mortality PV* Remdesivir 43.0%, control** 37.8%
24/10 USA authorizes the use of Remdesivir
Note 1) “National Health Institute, Report n.49/2020, 8/6/2020: “COVID-19: Interim Report on the definition, certification and classification of the causes of death”
According to this report the patients included in the 33.000 until 7/6/20 are composed as follows:
- Suspected case (without laboratory investigation: Author’s note)
- Someone with acute respiratory infection and with no other etiology, which completely explains the clinical presentation and with a travel or residence history with transmission of the virus.
- Someone with any acute respiratory Infection who has been in contact with a probable or confirmed case of Covid.
- Probable case: suspected case whose SARS-CoV-2 test result is doubtful or inconclusive (i.e. despite negative test the diagnosis is confirmed: Author’s note)
- Confirmed case. Case with laboratory confirmation independently of signs and clinical symptoms.
Note 2) “National Institute of Statistics” ISTAT Report from 16/7/20: “Impact of the Covid-19 epidemic on Mortality: Causes of death of positive deceased from SARS-CoV-2”
The report includes 4,942 statements of death submitted to the National Institute of Health with confirmed SARS-CoV infection. This constitutes only 15.6% of the reported cases until 25/5/20 out of a total of 31.573 deaths. Therefore the remaining cases are suspected or probable cases (i.e.with no laboratory diagnosis).
The statistical elaboration of this small group of patients has emphasised that: “Covid-19 is the directly responsibile cause of death in 89% of deaths of people positive to SARS-CoV-2”, a statement which is repeated daily like a prayer wheel.
Definition of directly responsibile for death: death is caused directly by Covid-19, when death would not have been verified, if the SARS-Cov-2 infection had not intervened (although often overlapping other pre-existing illnesses and their complications).
Note 3) The virological community should publicly release the same declaration as Frege on 16/6/1902 (modified by vaso di pandora): “Hardly anything more unwelcome can befall a scientific writer (virological community) than that one of the foundations of his edifice be shaken after the work (program for the “fight” against the pandemic) is finished. This is the position into which I was put (still Frege) by a letter from Mr Betrand Russell (Wegener der Weltbildzertruemmerer), as the printing of this volume (Public Measures against the Pandemic) was nearing completion.
Bibliography
- European Centre for Disease Prevention and Control: Using the masks in the Community. https://www.ecdc.europa.eu/en/publications-data/using-face-masks-community-reducing-covid-19-transmission
- Ministero della Salute Italiano: Covid-19: Situazione in Italia al 4/11/2020. http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?area=nuovoCoronavirus&id
- Vaso di Pandora: Aerosol als der einzig relevanter Uebertragungsweg des Coronavirus: epidemiologische Analyse, 29/05/2020. https://www.vasodipandora.net/2020/05/29/aerosol-als-der-einzig-relevanter-uebertragungsweg-des-coronavirus-epidemiologische-analyse/
Vaso di Pandora: L’aerosol quale unica via rilevante di trasmissione del coronavirus: evidenze epidemiologiche, 24/05/2020. https://www.vasodipandora.net/2020/05/24/laerosol-quale-unica-via-rilevante-di-trasmissione-del-coronavirus-evidenze-epidemiologiche/
- Vaso di Pandora: Wegener, der Weltbildzertruemmerer, 29/05/2020 https://www.vasodipandora.net/2020/05/29/der-weltbildzertruemmerer-wegener-und-das-coronavirus/
Vaso di Pandora: Considerazioni generali sul coronavirus, 25/05/2020- https://www.vasodipandora.net/2020/05/25/considerazioni-generali-sul-coronavirus/
A) Ministero della Salute Italiano: Covid-19: Situazione in Italia al 4/11/2020. http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?area=nuovoCoronavirus&id
B) Istituto Nazionale di Statistica; decessi e cause di morte. 4/11/2020 https://www.istat.it/it/archivio/240401#:~:text=Decessi%20e%20cause%20di%20morte%3A%20cosa%20produce%20l%E2%80%99Istat,da%20fonte%20anagrafica%2C%20con%20cadenza%20mensile%20ed%20annuale.
C) John P. A. Ioannidis, Bulletin of the WHO: Infection fatality rate of COVID-19 inferred from seroprevalence data, 14/10/2020. https://www.who.int/bulletin/online_first/BLT.20.265892.pdf
D) Istituto Superiore della Sanità (ISS): COVID-19: rapporto ad interim su definizione, certificazione e classificazione delle cause di morte, n.49/2020. 8/6/20
E) Istituto di Statistica Italiana: Impatto dell’epidemia COVID-19 sulla mortalità: cause di morte nei deceduti positivi a SARS-COV-2, https://www.istat.it/it/archivio/245573
F) Alta Scuola di Economia e Management dei Sistemi Sanitari (ALTEMS): Interim analysis sull’impatto economico per l’Ssn del Covid-19, 28/05/2020, https://altems.unicatt.it/altems-flash%20report%20altems.pdf
G) Das Handelsblatt: Coronakrise rettet die Kliniken – aber die Pleitegefahr bleibt hoch, 18/06/2020, https://www.handelsblatt.com/technik/medizin/krankenhausmarkt-coronakrise-rettet-die-kliniken-aber-die-pleitegefahr-bleibt-hoch/25928050.html?ticket=ST-8782875-ukG7jD77bEeYcW6Kezpt-ap2
H) WHO Solidarity trial consortium: Repurposed antiviral drugs foe COVID-19 – interim WHO SOLIDARITY trial results, 15/10/2020, https://www.medrxiv.org/content/10.1101/2020.10.15.20209817v1.full.pdf
I) The Recovery Collaborative Group: Dexamethasone in hospitalized Patients with Covid-19 – Preliminary Report, 17/07/2020, https://www.nejm.org/doi/full/10.1056/NEJMoa2021436
J) European Medicines Agency: Guidance on the Management of Clinical Trials during the COVID-19 (Coronavirus) pandemic, 28/4/20, https://ec.europa.eu/health/sites/health/files/files/eudralex/vol-10/guidanceclinicaltrials_covid19_en.pdf
K) European Commission: European Commission secures EU access to Remdesivir for treatment of COVID-19, 29/07/2020, https://ec.europa.eu/commission/presscorner/detail/en/ip_20_1416
L) Plenardebatte 07/03/2011 – Umgang mit der H1N1 – Grippe (Europaeische Union), https://europarl.europa.eu/sides/getDoc.do?pubRef=-//EP//TEXT+CRE+20110307+ITEM-023+DOC+XML+V0//DE
M) Transparency Intenational: Transparency Deutschland fordert Aufarbeitung des Schweinegrippen-Fehlalarms, 07/10/2011, https://www.transparency.org/en/press/20111007-schweinegrippe
N) Europaeischer Rechungshof: Interessenkonflikte wurden von den ausgewaehlten Agenturen nicht angmessen gehamdhabt, 11/10/2020. https://ec.europa.eu/commission/presscorner/detail/de/ECA_12_39
O) Gottlob Frege: Eine Einfuehrung in sein Werk, Walter de Gruyter – Berlin – New York 1989, https://books.google.it/books?id=du2_q1PRTRAC&pg=PP5&source=kp_read_button&redir_esc=y#v=onepage&q&f=false